Legionellosis and Recent Advances in Technologies for Legionella Control in Premise Plumbing Systems: A Review




1
United States Environmental Protection Agency, Office of Research and Development, 26 W. Martin Luther King Dr., Cincinnati, OH 45268, USA
2
Department of Chemical and Environmental Engineering, University of Cincinnati, Cincinnati, OH 45268, USA
*
Authors to whom correspondence should be addressed.
Water 2020, 12(3), 676; https://doi.org/10.3390/w12030676
Submission received: 30 December 2019
/
Revised: 20 February 2020
/
Accepted: 21 February 2020
/
Published: 2 March 2020
(This article belongs to the Special Issue Removal and Inactivation of Waterborne Pathogens during Water Treatment Processes)
Abstract
:This review discusses Legionella, among the most prolific and publicly well-known waterborne pathogens, and advances in potential treatment technologies. The number of cases associated with Legionella continues to rise, as does its public awareness. Currently, cases associated with premise plumbing account for the largest number of legionellosis cases in the United States. So, while it is important to understand Legionella as such, it is also important to investigate how to treat drinking water in premise plumbing for Legionella and other waterborne pathogens. While there are currently several methods recognized as potential means of inactivating waterborne pathogens, several shortcomings continue to plague its implementation. These methods are generally of two types. Firstly, there are chemical treatments such as chlorine, chlorine dioxide, monochloramine, ozone, and copper-silver ionization. Secondly, there are physical treatments such as thermal inactivation and media filtration. Their shortcomings range from being labor-intensive and costly to having negative health effects if not properly operated. Recently developed technologies including ultraviolet (UV) irradiation using light emitting diodes (LEDs) and innovative carbon nanotube (CNT) filters can better control waterborne pathogens by allowing for the simultaneous use of different treatment measures in plumbing systems.
1. Introduction
Legionnaires’ disease (LD) and the waterborne pathogen associated with it have continued to garner the attention of the public, health professionals, and regulating bodies alike since its initial outbreak in 1976, demonstrated by the recent increase in public health guidance and policy [1,2,3,4,5,6,7]. According to data reported to the Centers for Disease Control and Prevention (CDC) through the National Outbreak Reporting System, there were 41,269 outbreaks of Legionnaires’ disease in the United States (U.S.) between 1998 and 2014, with the incidence rate thought to be somewhere between 7.0 and 7.9 cases per 100,000 people [8,9]. Furthermore, Legionnaires’ disease is a financial burden, with hospitalizations due to Legionella spp. costing nearly 434 million dollars annually in the U.S. [10]. Although the first outbreak of Legionnaires’ disease occurred in the U.S., it affects many countries across the world at the same incidence rate. Data reported to the European Centre for Disease Prevention and Control (ECDC) found an incidence rate of 1.3 cases per 100,000 for 2015 [11]. This is comparable to the rate reported to the CDC, meaning there is a similar incidence rate in both the U.S. and Europe [11]. Australia also demonstrated a similar incidence rate in 2009, at 1.8 cases per 100,000 people [12].
While Legionella spp. is found in both natural and artificial environments, most cases of disease are linked to man-made systems [13]. In particular, premise plumbing (e.g., showers, toilets, and sink faucets) and the water systems associated with it, including cooling towers, whirlpools, mist machines, and decorative fountains, are the most common sources of Legionella transmission [14,15,16,17,18] (Figure 1). A Legionella infection can result from exposure to aerosols and aspiration, and Hamilton et al. identified showers as the main exposure route of Legionella for indoor residential water uses [19].
Since most cases of Legionnaires’ disease stem from premise plumbing, studies have focused on methods to inactivate or remove this pathogen in order to mitigate the risk [18]. Currently, there are six technologies citied by the U.S. Environmental Protection Agency (EPA) that can be used for control of Legionella: chlorine, chlorine dioxide, monochloramine, copper-silver ionization (CSI), ozone, and ultraviolet (UV) disinfection [20]. However, the effectiveness of each of these methods can vary, and some of them have negative effects associated with their use [20]. For instance, the three commonly used variations of chlorine (i.e., free chlorine, chlorine dioxide, monochloramine) result in the formation of disinfection byproducts (DBPs) and can cause corrosion of plumbing [20,21,22,23,24]. CSI can result in negative aesthetic effects on water and adverse health effects if high levels of these chemicals are ingested [25,26,27]. Ozone can also result in the formation of disinfection byproducts, but does not result in a disinfectant residual [20,24]. UV disinfection does not provide an effect on water downstream of the unit and can result in mercury contamination if the lamp breaks; however, it does not result in any negative health effects or DBPs [20,28,29]. Light emitting diodes (LEDs), a novel emerging technology, may be able to help overcome the shortcomings of traditional lamps, as they do not contain mercury [30]. LEDs are also more compact and durable than mercury lamps, which may allow for them to be used at the point-of-use (POU) [31]. A further literature review on this emerging technology, as well as the six most commonly used treatment practices, are presented in the following sections.
2. Legionella and Legionellosis
2.1. Outbreaks of Legionellosis
Most infectious diseases are discovered in the wake of an outbreak; Legionnaires’ disease is no exception [1]. In the 1960s, an unknown type of pneumonia broke out in several places, but most cases could not be traced back to a specific type of bacteria [32,33]. In July of 1976, at a convention of the American Legion in Philadelphia, Pennsylvania, there was another outbreak of illness stemming from an unknown cause [1]. Following the outbreak of Legionnaires’ disease in 1976, an extensive analysis was performed to determine the causative agent; eventually, it was established that the same pathogen was responsible for both Pontiac fever (PF)—named after the city of Pontiac, MI—and LD [34]. Outbreaks of legionellosis, the term used to collectively describe LD and PF, have continued since its discovery 35 years ago [35].
One of the more recent outbreaks of Legionnaires’ disease occurred in Genesse County, within which lies the city of Flint, MI [36]. In 2014, the city of Flint changed its water source from Lake Huron to the Flint River to cut down on costs [37]. Following the switch of the city’s water source, two separate outbreaks of Legionnaires’ disease followed: one from June 2014 to March 2015 and the other from May 2015 to December 2015 [36,38]. During the first outbreak, there were 45 confirmed cases of LD reported, with seven deaths [36]. The following year, during the second outbreak, an additional 46 cases of LD were reported, with seven more fatalities [38]. In both outbreaks, a Genesee County hospital was implicated as the potential source. In the two weeks prior to development of the disease, 51% of the cases in the first outbreak and 58.7% of the cases in the second outbreak had been to this particular facility [36,38].
While outbreaks continue to occur, other sporadic cases are also common [39]. According to data reported by the CDC, the number of legionellosis cases has increased 217% from 2000 to 2009 in the U.S., with 99.5% of reported cases causing LD and 0.5% of the cases causing Pontiac fever [40]. However, the amount of cases reported by the CDC may be an underrepresentation of the actual number of cases [8]. A study conducted in 1991 recorded every case of pneumonia in two counties in Ohio, and this study was considered to be a good representation of the U.S. [8]. The incidence rate for pneumonia caused by LD was between 7.0 and 7.9 cases per 100,000 people, meaning that there would be between 8,000 and 18,000 cases annually in the U.S. [8]. This is a stark contrast from the number of cases reported by the CDC for the same year. In 1991, there was an incidence rate of 0.53 cases per 100,000 people, and 605 people were diagnosed with legionellosis [41]. Therefore, the number of cases reported by the CDC may be less than 10% of the actual cases. Not only does LD affect the health of a potentially large number of people in the U.S. annually, but it also bears a large financial burden [10]. The total cost of hospitalizations attributed solely to LD is estimated at over 433 million dollars, costing on an average 33 thousand dollars per hospital stay [10].
LD is not limited to the U.S. Europe also has a large number of cases reported annually [11,42]. Due to its high and increasing prevalence, 36 countries united to form the European Working Group for Legionella Infections to monitor its trends [42]. Data from this group report that the incidence rate from 1993 to 2008 has nearly tripled, from 0.41 cases per 100,000 people to 1.18 cases per 100,000 people [42]. More recent data report that the rate of all cases increased from 0.97 cases per 100,000 people in 2011 to 1.30 cases per 100,000 people in 2015 [11]. Australia has also formed a network that allows for the monitoring of legionellosis [12]. In 2014, the most recent year that data are available, there were 424 cases [12]. Similar to other geographic regions, Australia experienced an increase in the number of cases of legionellosis reported from 2009 to 2014 [12]. Since legionellosis continues to affect many people both domestically and abroad, it is important to understand the responsible etiologic agent.
2.2. Causative Agent of Legionellosis: Legionella
After the 1976 outbreak of LD, a bacterium was isolated in lung samples from patients, and the isolated bacteria were unknown bacilli that ranged from 0.4 µm to 0.8 µm in width and ranged from 2 µm to 4 µm in length [43]. A number of standard tests were run, including Gram staining to identify the responsible etiological agent [44]. However, the bacteria were not successfully stained, as only some stained faintly as Gram-negative rods [45]. Since the bacteria was not identified upon examination, a large relatedness study commenced following the 1976 outbreak [46]. This study compared twelve unknown bacterial strains suspected to cause LD to strains of known and well-characterized bacteria [46]. However, it was determined that the strains were not related to any of these microorganisms [46]. This result suggested that the unknown bacterial isolates were either members of an understudied species or a previously unclassified group [46].
Further research found defining characteristics that excluded the unknown bacteria from other classified families [47]. The unidentified bacteria were fastidious, required cysteine, incapable of reducing nitrates, negative for degrading urea, and required some oxygen to grow [48]. Based on both these characteristics and the results of the relatedness study, the disease-causing bacteria were determined to be part of a novel family [47]. The proposed name was Legionella pneumophila, with the genus name referring to the American Legion, where the disease was first discovered, and the species name roughly translating to “lung-loving [47].” L. pneumophila was the first species in the newly classified family Legionellaceae [47].
Members of the genus Legionella can be found in nearly all aquatic environments, including lakes, premise plumbing, and even in rainforest canopies [49]. While Legionella thrive in a specific temperature range or at a certain pH, this pathogen can survive in temperatures from 0 °C to 68 °C and in a pH range of 5.0 to 8.5 [49]. Although this microorganism can be found in a variety of natural settings, including lakes and ponds, most cases of legionellosis are linked back to premise plumbing and the water systems associated with it [18]. There are documented outbreaks stemming from air conditioning units [34], cooling towers [14,44,50,51,52,53,54,55], decorative fountains [16,56,57], grocery store mist machines [15], and whirlpool spas [17,58].
While Legionella are fastidious microorganisms which require special nutrients to grow, they have evolved to thrive in a variety of artificial environments, including mechanisms that allow them to take advantage of other microbes present in water [59,60]. Specifically, Legionella can infiltrate biofilms found in premise plumbing. One study determined that this pathogen can colonize a biofilm successfully in two hours [61]. Furthermore, another study sampled ten biofilms from different cooling towers and determined that L. pneumophila was present in all samples [62]. While biofilms are found in a number of aquatic environments, those associated with warm or hot water systems yield the greatest risk of being colonized by Legionella [63]. There are over 300 reports of LD occurring in premise plumbing water systems found in various peer-reviewed literature and public-health reports [64].
Since this pathogen cannot replicate without all of its required nutrients, it developed an adaptation that allows it to infect amoebae [65]. This novel mechanism, termed coiling phagocytosis, is specific to Legionella [66]. After undergoing this novel type of phagocytosis, the bacteria are enclosed within a membrane-bound cytoplasmic vacuole [66]. Traditional phagocytosis entails symmetrical edges engulfing the bacteria, while coiling phagocytosis involves the pseudopod both interacting with and rolling into itself, creating a whorl [67]. This special type of phagocytosis is thought to assist in uptake, as it may allow for the more effective invasion of amoebae [67]. Typically, Legionella only multiply extracellularly in the presence of complex media, however, intracellular reproduction can occur while undergoing phagocytosis [68]. Therefore, by undergoing coiling phagocytosis and infecting amoebae, Legionella thrive in environments that may not readily contain all of its growth requirements [68]. When the nutrients from the host cell become limited, these bacteria lyse the host and re-enter the aquatic environment [69].
Due to the etiological ramifications of Legionella, it is important to be able to detect its presence in premise plumbing and related water systems. Currently, there is a variety of methods used to detect this waterborne pathogen [60]. Traditional culture using Buffered Charcoal Yeast Extract Agar (BCYE) is considered the ‘gold standard’ to determine the presence of Legionella from both clinical and environmental samples [70]. However, due to the slow growing nature of Legionella, results take at least five days to obtain [70]. The traditional culture method can be coupled with other treatments and additives to the BCYE agar to make culturing this organism easier, because BCYE is prone to overgrowth by non-target bacteria that obscure Legionella colonies. Isolates from BCYE plates need to be confirmed as Legionella by streaking onto BCYE plates without L-cysteine, and then further identified as L. pneumophila using latex agglutination tests specific for L. pneumophila. Another culture-based method developed by IDEXX laboratories (Westbrook, MA, USA) called Legiolert [71] detects L. pneumophila-only strains in potable and non-potable water sources. While this method is relatively simplistic and less laborious than the traditional culture method, it takes a full seven days to determine if the sample is positive for the presence of L. pneuomphila. As mentioned above, one major issue with other culture methods is overgrowth of non-target organisms. The manufacturer claims that this product selectively grows L. pneumophila even in the presence of other non-target organisms. However, further testing against various types of environmental water samples using this method needs to be done to ensure its reliability due to its novelty [72,73]. Other methods, such as direct fluorescent antibody staining, indirect immunofluorescence assays, and rapid microagglutination tests, are less laborious ways to detect Legionella, although they are not as sensitive or specific as the culture method [70]. Another common detection method for suspected clinical cases is a urinary antigen test, which has both high specificity and sensitivity [37]. However, because only 80% of patients with legionellosis excrete the antigen through urine, this method cannot always achieve a proper diagnosis [37]. Polymerase chain reaction (PCR) is used for both clinical and environmental samples, with 100% specificity [37]. Furthermore, PCR identifies specific serogroups of a species of Legionella, but can be relatively expensive and does not differentiate between live and dead cells [37]. While there are a number of methods used to identify the presence of Legionella in both clinical and environmental samples, the culture is still considered optimal.
2.3. Species, Serogroups, and Strains of Legionella
More than fifty known species have been added to the Legionellaceae family since its initial characterization in 1978, with some species further subcategorized into different serogroups [46,64]. Of these species, however, less than half of them—around twenty—have been linked to cases of disease [74]. One study analyzed cases of Legionnaires’ disease using data from the U.S., Italy, Switzerland, Australia, and New Zealand to determine what species were most commonly cited as the cause [74]. The findings determined that, across all of the countries analyzed, the same three species were responsible for the majority of the cases: L. pneumophila, Legionella micdadei, and Legionella longbeachae [74]. However, there was a difference in the percentage of cases attributed to each species [74]. L. pneumophila was responsible for 88.2% of cases in the U.S. and European countries [74]. In New Zealand and Australia, however, the same species caused 45.7% of cases with L. longbeachae responsible for 30.4% of cases [74]. This study suggested that there may be either a difference in distribution of species, with some being more prevalent in some countries compared to others, or a difference in virulence, as L. longbeachae may have an evolved mechanism that leads to increased virulence in some geographic locations [74].
Three different species are commonly cited as causing the majority of LD cases. Within these species, specific serogroups are linked to more cases than others [75]. For example, one study analyzed cases of Legionnaires’ disease reported to the CDC from 1980 to 1989 and found L. pneumophila was responsible for nearly 95.4% of all cases [75]. Specifically, L. pneumophila serogroup 1 was the cause of 59.3% of all Legionnaires’ disease cases reported during this time period [75]. Reported LD cases were confirmed by at least one type of diagnostic testing method (e.g., urinary antigen test (UAT), serology, and culture). It should be noted that most cases (>97%) are confirmed by UAT for L. pneumophila serogroup 1 rather than culture. More recently, the CDC reported that about 35% of culture-confirmed cases from 2014 to 2015 were not identified to a specific species, suggesting underestimation of unidentified species responsible for LD cases. Similarly, of the 3645 culture-confirmed cases of LD reported to the European CDC from 2011 to 2015, 3511 (96.3%) were due to L. pneumophila, including 3020 (82.9%) due to L. pneumophila serogroup 1 [11]. However, even within this serogroup, virulence seems to vary [76]. One study examined the number of cases caused by two different strains of L. pneumophila serogroup 1 [76]. The study examined two nearby hospitals that were well-colonized with different strains of L. pneumophila serogroup 1 [76]. Between those two similarly situated hospitals, one hospital reported only one case of nosocomial pneumonia, while the other hospital had nineteen cases [76]; since both hospitals were similarly colonized and the facilities were considered to have the same risk factors, the results of this study suggest that virulence can vary greatly even within the same serogroup [76]. As there is variety in the characteristics and virulence of different strains of Legionella, one strain may not be representative of the entire species, let alone the species.
3. Current Technologies for Control of Legionella in Premise Plumbing Systems
Since premise plumbing and its associated water systems are the main mechanisms of human exposure, effectively inactivating Legionella in drinking water is important. According to a recent U.S. EPA report [20], six candidate treatment technologies to control the risks from Legionella bacteria in premise plumbing systems are commonly applied (Figure 2). In addition to these six technologies, in this section, we discuss two other available treatment processes.
3.1. Chemical Treatment Technologies
3.1.1. Chlorine-Based Disinfection
Three different types of chlorine such as free chlorine, monochloramine, and chlorine dioxide are widely used to inactivate pathogens in drinking water treatment in the U.S. [77]. Chlorine inactivates pathogens by interacting with the cell membrane, resulting in the leakage of macromolecules from the cell [78]. This leakage then causes changes in the physical, chemical, and biochemical processes that take place inside the cell [78].
(1) Free chlorine: One study examined the effectiveness of two concentrations of free chlorine, 0.2 mg/L and 0.5 mg/L, on different strains of Legionella [77]. Table 1 depicts the amount of time required to achieve a 4-log reduction [77]. While these concentrations are much lower than the U.S. EPA guideline of 4.0 mg/L as a running annual average [79], they are reflective of levels that would be commonly found in hot water loops of premise plumbing [78]. At the lower concentration of free chlorine, neither strain of L. pneumophila serogroup 1 achieved the 4-log reduction in the 24-min time frame tested [77]. While the two L. pneumophila serogroup 1 strains reached the desired decrease at the higher concentration of free chlorine, both the laboratory and environmental strains required a longer contact time than the other serogroups and species tested [77]. Furthermore, the laboratory strain required twice the amount of time to achieve the same reduction when compared to the environmental strain, demonstrating that there can be variance within a single serogroup regarding the efficacy of inactivation [77].
In addition to laboratory experiments, Orsi et al. investigated the effectiveness of free chlorine on premise plumbing systems that were well-colonized with Legionella [80]. For continuous hyperchlorination, the concentration of chlorine was targeted to be between 0.5 mg/L and 1.0 mg/L of free chlorine [80]. The results of the study are summarized in Table 2. Briefly, it was determined that continuous hyperchlorination resulted in significantly fewer positive sites [80]. However, even after this treatment method was in place for five years, there were still sites that tested positive for Legionella, suggesting that this technology could not completely control for Legionella [80].
Physicochemical parameters such as chlorine concentration, pH, temperature, turbidity, and concentration of natural organic matter (NOM) affect the efficacy of chlorination. Under typical drinking water conditions, the microbial inactivation efficacy of chlorine is increased at lower pH. Two main species of free chlorine include hypochlorous acid (HOCl) and hypochlorite ion (OCl−). The former is the stronger oxidant, and the ratio of these two chlorine species is dependent on water pH (i.e., HOCl dominates at pH < 7 and OCl− dominates at pH > 7). In chlorinated water distribution systems, typical water pH is >7, diminishing the efficacy of chlorine disinfection in practice. While the bactericidal action of chlorine is enhanced at a higher temperature, it is difficult to maintain chlorine residuals in hot water systems due to rapid degradation of free chlorine [81].
Chlorine provides a disinfectant residual to inhibit microbial growth in a premise plumbing system. However, one of the biggest potential water quality issues in chlorinated water is the formation of carcinogenic disinfection byproducts (DBPs) such as trihalomethanes (THMs). Loret et al. reported that total THM levels exceeded the EPA drinking water standard of 80 μg/L in water plumbing systems with an applied chlorine dose of 2 mg/L [82]. In addition, chlorination at high levels in premise plumbing systems can contribute to corrosion in high density polyethylene (HDPE) and copper pipes, suggesting the addition of corrosion-inhibiting chemicals (e.g., phosphate and silicate) [82,83,84].
While several studies demonstrated that chlorine is very effective to inactivate planktonic Legionella in water [85], it is much less effective at penetrating established biofilms and at controlling Legionella associated with biofilms [82,86]. Extracellular polymeric substances (EPS) are produced by microorganisms, and its production is enhanced under stressful environmental conditions. It is well documented that EPS can react with chlorine before the disinfectant reaches microorganisms in the biofilm [87]. Moreover, Fisher et al. demonstrated that chlorine-wall decay rates increase at lower chlorine residuals (below 0.5 mg/L) using accurate mathematical modeling [88]. In addition to the fate of chlorine, interaction of Legionella with co-occurring amoebae increases the resistance of Legionella to chlorine [89].
(2) Chlorine dioxide: Other forms of chlorine are also being examined as possible technologies to control for Legionella present in drinking water [20]. Chlorine dioxide has relatively high oxidation potential to inactivate various waterborne pathogens [90] and can be effectively applied over a wider pH range, compared to other forms of chlorine [91]. The addition of chlorine dioxide is one alternative, with the mechanism of inactivation relying on its ability to easily diffuse through cell membranes of microorganisms and oxidize cellular components [20]. A recent study investigated the effectiveness of chlorine dioxide for inactivation of L. pneumophila. For this experiment, the log inactivation of L. pneumophila at different contact times was determined, both alone or co-cultured with different amoeba [92]. The initial concentration of chlorine dioxide was 0.4 mg/L, with the results of this study showing that L. pneumophila exposed to chlorine dioxide at this concentration can achieve a 4-log reduction with a contact time of approximately 2 min (i.e., <1 mg min/L) [92]. There was a significant reduction in the log-number of L. pneumophila when co-cultured with various amoeba, suggesting it may be an effective technology to control for the presence of Legionella in premise plumbing [92]. Furthermore, it appears to be superior in penetrating biofilms like monochloramine (NH2Cl) [91], and Loret et al. reported significant biofilm reduction as well as the effective control of Legionella in the pilot-scale pipe loop system [82]. Due to its success at inactivating Legionella in laboratory experiments, some facilities opted to install chlorine dioxide generators to remediate well-colonized premise plumbing systems [93].
One such study examined the percent positivity of distal sites for Legionella over 40 months after installation of a chlorine dioxide generator [93]. For this particular application, chlorine dioxide was injected into the cold water at a concentration between 0.5 mg/L and 0.7 mg/L [93]. Per U.S. EPA guidelines, no more than 0.8 mg/L of chlorine dioxide can be present in finished drinking water [94]. Following treatment, the cold water had Legionella positivity of less than 20%, with residuals averaging around 0.42 mg/L [93]. In the hot water, the residual was consistently around 0.7 mg/L, with the percent positivity less than 10% [93]. There were significant reductions in the number of positive samples when compared to the starting point; however, after 40 months of treatment, Legionella was still present in the system [93]. Chlorine dioxide does not produce high levels of chlorinated DBPs and is widely used as an alternative disinfectant to free chlorine since the promulgation of the total trihalomethanes (TTHM) regulation in the 1980s [95,96]. The main DBPs of chlorine dioxide disinfection include chlorite and chlorate which can cause anemia and an enlarged thyroid, respectively [24,97], and maximum contaminant level (MCL) of chlorite is 1.0 mg/L [22].
(3) Monochloramine is another form of chlorine being explored as a technology to mitigate the risk of Legionella in premise plumbing [20]. Like the other types of chlorine disinfectants, monochloramine (NH2Cl) is a colorless water-soluble liquid with the capability to maintain a disinfectant residual in premise plumbing systems. Monochloramine has been commonly used in drinking water treatment plants for more than 100 years, and the usage rate of monochloramine increased significantly since implementation of the Stage 2 Disinfectants and Disinfection Byproducts Rule (D/DBPR) [98]. While monochloramine penetrates biofilms relatively fast and limits Legionella growth effectively in premise plumbing [99], Herath and Sathasivan recently reported chloramine stress induces the production of the chloramine decaying proteins (CDP) in biofilm which accelerate the decay of chloramine [100].
The mechanism of inactivation involves the inhibition of proteins or of protein-mediated processes [90]. Laboratory experiments were conducted to determine the efficacy of inactivation [101]. For this study, a 4-log reduction was achieved at the initial concentration of 0.8 mg/L of monochloramine after a contact time of ~27 min, demonstrating that monochloramine can be an effective technology for inactivating Legionella [101]. Monochloramine was also successful at inactivating L. pneumophila co-cultured with different amoeba [101]. One full-scale study analyzed the effectiveness of continuous injection of monochloramine in premise plumbing systems at levels between 1.5 mg/L and 3.0 mg/L [101]. As seen in Table 3, monochloramine was successful at limiting the number of positive samples, as there were significantly fewer sites that tested positive for Legionella after treatment when compared to those before treatment [101].
It is well documented that chloramination reduces the formation of chlorinated DBPs such as THM and haloacetic acid (HAA). However, chloramine species, including monochloramine, are commonly associated with the formation of disinfection byproducts such as chlorates and N-nitrosodimethylamine (NDMA), which may be carcinogenic to humans [102]. The United States Environmental Protection Agency (USEPA) monitors NDMA as part of an unregulated contaminant monitoring (UCMR); results indicate that NDMA was detected in about 10% of samples from public water systems [103]. According to the USEPA, a 1 × 10−6 cancer risk level and a screening level of tap water for NDMA are 0.7 and 0.42 ng/L, respectively [104,105].
Several operational practices need to be considered for successful application of monochloramine in premise plumbing systems: (1) chlorine-to-ammonia ratio; (2) appropriate pH; (3) chloramine residual maintenance; and (4) monitoring water chemistry such as organic nitrogen. Monochloramine can cause pipe corrosion and degradation of rubber and plastic material in a premise plumbing system like other chemical disinfectants [21,82,106]. The concentrations of monochloramine maintained in the systems range between 1.0 and 4.0 mg/L, and the ratio of chlorine-to-ammonia is 3:1 to 5:1. Monochloramine is relatively stable under varying temperature and much more effective in maintaining disinfectant residual than free chlorine in hot water [107]. Since relatively high prevalence of Legionella has been observed often in hot water possibly due to lack of disinfectant residuals, monochloramination would be a useful tool to control Legionella in premise plumbing systems.
3.1.2. Copper-Silver Ionization (CSI)
Other methods are being explored as possible alternatives because of the shortcomings associated with each of the aforementioned chlorine species. One disinfection strategy that is commonly used in premise plumbing systems with hot water recirculating loops, particularly hospitals, is CSI [91,108]. In order to determine whether copper ions, silver ions, or a combination of the two are effective at inactivating Legionella, different concentrations were tested in a laboratory setting to determine the log inactivation [109]. While both copper and silver ions were used to successfully reduce the levels of Legionella, when used together, they created a synergistic effect, resulting in a higher inactivation rate [109]. The mechanism behind this inactivation involves the copper ions reacting with and destroying the cell wall permeability, which allow the silver ions to interfere with the synthesis of proteins and enzymes [109].
In addition to laboratory experiments, disinfection units that produce copper and silver ions have been installed in various facilities. Walraven et al. studied the effectiveness of CSI in five different buildings by tracking the Legionella positivity percentage [110]. Two of the facilities had data regarding the percent positivity before the installation of the units, with both experiencing significant decreases in the positivity of Legionella [110]. Of the sites that were monitored strictly after installation, the majority had low levels of positivity with less than 100 colony forming units (CFU)/mL in drinking water and less than 1000 CFU/mL in cooling water [110]. The average injection level of copper and silver ions was 357 µg/L and 33 µg/L, respectively [110]. However, the measured levels at distal points in the systems were 296 µg/L and 20 µg/L of copper and silver, respectively [110]. One of the major challenges facing CSI is ensuring that the added ions are flushed throughout the water distribution system. This study found that decreased levels may have contributed to increased positivity at distal points in the system. Another issue associated with CSI is that Legionella may develop resistance to copper and silver ions [25].
Physicochemical parameters are critical for the efficacy of CSI treatment in terms of the speciation of both metals in water. The higher levels of both metal ions, the better treatment effectiveness. While pH plays an important role in the speciation of copper (i.e., copper ion levels decrease significantly under alkaline pH), silver ions are relatively stable in the pH range of 6–9. Some chemical parameters (e.g., chloride and phosphates added for chlorination and corrosion control, respectively) react with copper and silver ions, and consequently these metal complexes diminish their microbiocidal power [111,112,113]. Moreover, the latter metal complex chlorargyrite (AgCl(s)) contributes to the purple/grey stains in bathroom porcelain [114]. Other physicochemical parameters such as organic carbon, calcium, magnesium, bicarbonate, and temperature do not appear to impact the treatment efficacy of CSI [112]. In addition to its treatment efficacy, Zhang and Andrews reportedaccelerated chlorine decay and increased disinfection byproduct formation at pH 8.6 in the presence of copper ions and natural organic matter [115]. CSI may result in corrosion under some conditions in water plumbing similar to other chemical disinfectants (e.g., chlorine, chloramine, chlorine dioxide, and ozone) [82,116,117].
3.1.3. Ozonation
Ozonation is another method used to treat pathogens that are present in water, as it has two different mechanisms used for inactivation [118]. First, ozone oxidizes the sulfhydryl groups and amino acids of a variety of cell components, such as enzymes, peptides, and proteins, and creates shorter peptides [118]. Secondly, ozone oxidizes polyunsaturated fatty acids to acidic peroxides, causing degradation of the cell envelope [118]. Together, these mechanisms disrupt the cell and result in leakage of the cellular contents [118]. Domingue et al. examined the effectiveness of ozone on L. pneumophila serogroup 1 at different levels of pH and temperatures [119]. The log inactivation at each of the tested levels is shown in Table 4 [119]. All the various combinations achieved at least a 2-log reduction, showing that ozone is an effective method at inactivating L. pneumophila [119].
Another study analyzed the effect of ozonation on a premise plumbing system over the course of three years; the results are shown in Table 5 [120]. When compared to the previous three years, there was not a significant decrease in the percent of positive samples [120]. Furthermore, the average concentration of Legionella present in the positive samples was not significantly different before and after ozonation [120]. Therefore, ozonation was not an effective remediation strategy for this premise plumbing system [120].
The efficacy of ozonation to inactivate various waterborne pathogens including UV-resistant adenovirus and chlorine-resistant protozoan parasites outpasses most disinfection tools, suggesting an effective primary disinfectant [121,122]. However, ozone has limited its use as a secondary disinfectant because it is not feasible to maintain a residual due to its rapid decay rate under typical tap water conditions [121,122]. Ozonation can produce bromate while treating water-containing inorganic bromide. The MCL of bromate is 10 μg/L. The efficacy of ozonation mainly depends on (1) its decay rate and (2) disinfection efficiency. As water temperature increases, the disinfection efficiency increases, but the ozone decomposes faster (i.e., consequently lower contact time). For other operational conditions, the ozone decomposes faster at a higher pH, and slower with increasing alkalinity.
3.2. Physical Treatment Technologies
3.2.1. Thermal Inactivation
Another way of inactivating waterborne pathogens is increasing the temperature of the water. The increased temperature denatures the proteins, nucleic acids, and ribosomes inside the cell, resulting in cell death [123]. One study examined the amount of time that certain temperatures require to achieve a 4-log reduction of various strains of Legionella; the results are visible in Table 6 [77]. For all strains, the higher temperatures tested resulted in shorter time periods required to reach a 4-log reduction of Legionella when likened to the lower temperatures [77]. Comparing two strains of L. pneumophila serogroup 1 showed a significant difference in the amount of time required to achieve a 4-log reduction at 50 °C and 55 °C, thus showing that the efficacy of inactivation varies across different strains [77]. While the desired level of inactivation was achieved in nearly a minute at 70 °C, heating domestic water to this temperature in various facilities is usually not achievable [77,124]. International Building Code limits hot water temperature to be no greater than 120 °F (~50 °C) at the first outlet of a plumbing system [124]. At this temperature, some strains of Legionella require nearly an hour to achieve a 4-log reduction, which may not be attainable in the time that the water travels from the hot water heater to the first outlet [77]. While a thermostatic mixing valve would lower the required time period by allowing for the set point of the water heater to be higher, these pieces of equipment can be burdensome to maintain properly [31]. Furthermore, in the case of failure with these devices or conducting emergency disinfection using superheat-and-flushing, there is an increased risk of scalding due to the heightened temperatures of the water [124].
Mouchtouri et al. investigated the effectiveness of heat flushing on 497 different premise plumbing systems, including hospitals, hotels, and sports venues [125]. For this thermal disinfection study, the water at the heater was increased to between 70 °C and 80 °C, with temperatures at the faucets not falling below 65 °C [125]. The outlets were then flushed for five minutes [125]. The study found a significant decrease in the number of water systems positive for Legionella [125]. However, there were some positive systems that required a second hot water flush. Even after the second flush, some facilities were again positive for the presence of Legionella [125]. While heat flushing was effective for a number of the facilities, not all sites experienced the same level of disinfection and the effects were not sustained over time [125].
3.2.2. Media Filtration
Point-of-use (POU) filtration can be used as a temporary measure for remediation situations when restricting tap water usage. There are two types of filters that are commonly used in premise plumbing: carbon filters and membrane filters [126,127]. Carbon filters are typically used at outlets designed for human consumption, as they remediate bad taste and odors by removing chlorine and other compounds in drinking water [113]. One study attempted to determine whether carbon filters were effective at removing Legionella and other heterotrophic bacteria by using lab-scale granular activated carbon (GAC) filters [127]. GAC uses adsorption as the primary mechanism for removing contaminants present in the water [127]. In this study, the GAC filters tested were exposed to water spiked with Legionella, and daily samples were taken for the following three weeks [127]. At the end of the study, Legionella was present on both the GAC filters and in the effluent [127]. Similarly, Molloy et al. evaluated three types of carbon filters for their removal efficacy of Legionella for six weeks [128]. Legionella was efficiently removed by about 8-log, but Legionella colonization on the filter media was observed and moreover, Legionella sloughed off over time. Thus, it was thought that this pathogen colonized the filter on both the GAC particles and the inner surface. Since Legionella colonizes the carbon filter while passing through, it is a challenging disinfection strategy that may result in a greater presence of the pathogen in drinking water.
Membrane filters have a different mechanism of removing pathogens from water than carbon filters [126,127]. Advances in membrane technologies improve the microbial removal efficacy and increase filter lifespan. Several studies reported that various kinds of membrane-based POU filters successfully controlled Legionella in hospital water systems with a filter lifespan of four to eight weeks [129,130,131]. Legionella and other pathogens can be colonized on the filter media, if the POU devices are not regularly replaced. Appropriate replacement rate is critical for microbial control. POU application can be implemented with primary treatment technologies as an additional barrier to control Legionella.
One study analyzed the effectiveness of this filter type in a hospital setting by adding filters to four faucets and having three faucets as controls without filters [126]. Samples were taken throughout two weeks to determine whether they successfully removed Legionella from the effluent [126]. The filters removed L. pneumophila completely, when compared to the controls with concentrations of around 100 CFU/mL [126]. While membrane filters are successful at removing Legionella, there are several practical shortcomings that make its implementation throughout a large premise plumbing system challenging. The effectiveness of filters depends mainly on the type of filter used [126,127].
3.3. Challenges in Physical and Chemical Treatments
The current physical and chemical treatment technologies discussed above have demonstrated effectiveness in regard to inactivating waterborne pathogens in premise plumbing systems [20]. However, each of those methods has drawbacks associated with it [20]. The usage of chemical treatment technologies as a way to inactivate waterborne pathogens in drinking water can result in potentially hazardous chemicals being added or formed when these chemicals react with other chemicals in the water [20]. Chlorine and monochloramine have maximum contaminant levels (MCL) of 4.0 mg/L, meaning that exceeding these levels can result in adverse health effects [22]. Being exposed to high levels of chlorine for extended periods of time can cause eye and nose irritation and stomach discomfort, while monochloramine can result in adverse health issues in addition to anemia [22]. Chlorine dioxide has an MCL of 0.8 mg/L, with exposure to levels above this potentially resulting in anemia and nervous system effects in infants and young children [22]. Monitoring the concentrations of copper and silver is critical to ensure levels approaching the MCL of 1.3 mg/L and the secondary MCL of 0.1 mg/L, respectively [25,132]. Exposure to copper at levels above its MCL can result in gastrointestinal distress for short-term exposure or liver and kidney damage for long-term exposure [22]. Silver levels up to the secondary MCL of 0.1 mg/L do not lead to the occurrence of argyria, which is the main symptom of silver toxicity [133]. Chlorine, monochloramine, and chlorine dioxide also react with compounds in the water to form a myriad of different disinfection byproducts, each with different health risks [20]. Therefore, use of these chemicals in drinking water, particularly premise plumbing applications, must be constantly monitored in order to ensure that both the disinfectants and their byproducts do not exceed EPA limits [20].
Another challenge associated with injecting different disinfectants into drinking water is ensuring that the residuals at distal outlets are significant enough to inactivate pathogens [20]. Therefore, outlets must be regularly flushed to ensure the disinfectant is present [20]. An additional shortcoming of using chlorine, monochloramine, or chlorine dioxide is that they dissipate in hot water, making a residual challenging to maintain [20]. This, coupled with the requirement of regular flushing, can make maintaining residuals at distal outlets in hot water premise plumbing systems very laborious and difficult [20]. Ozonation is also problematic as a disinfection strategy, as it does not maintain a residual [134]. Furthermore, studies on premise plumbing using ozonation as a technology for controlling the presence of Legionella have not shown promising results [134]. Therefore, it is not commonly used as a disinfectant in premise plumbing applications, even though it has proven successful at inactivating pathogens in a laboratory setting [120].
Different filters have successfully removed Legionella from drinking water; while membrane filters are effective, carbon filters appear to harbor Legionella with an increased concentration in the effluent [126,127]. However, membrane filters must be replaced at regular intervals, ranging from weekly to semiannually [126]. Furthermore, most filters rated for removing waterborne pathogens are designed for the POU, requiring one filter for each of the fixtures [126]. Therefore, replacing these filters can be both laborious and a financial burden, making it impractical to use filters as the sole disinfection strategy in large premise plumbing systems with a high number of fixtures [126].
4. Emerging Treatment Technologies
4.1. Ultraviolet (UV) Irradiation
Due to the shortcomings associated with chemical and physical technologies, alternatives are constantly being developed; one of these technologies is UV irradiation [135]. UV light causes the formation of intrastrand pyrimidine dimers in the DNA strands [77,136]. These dimers prevent DNA from properly replicating, thus causing cell death [77]. Knudson analyzed the effectiveness of UV irradiation in inactivating four different strains of L. pneumophila and L. longbeachae [135]. At a fluence of 50 J/m2, or 5.0 mJ/cm2, there was at least a 3-log reduction achieved for all strains and species tested [135]. The variation among strains and species was not considered significant; therefore, they all had the same sensitivity to UV [135].
Few studies have reported the efficacy of UV in controlling premise plumbing systems in hospitals [99,137,138]. Hall et al. examined its effectiveness in a hospital that was recently constructed [138]. After taking regular samples and testing for Legionella over 13 years, there were no positive environmental samples [138]. Data pooled from other hospitals showed a 51% positivity rate, which is significantly greater than zero percent positivity rate at the hospital with the UV lamp at the point-of-entry [138]. Furthermore, the facility across the street experienced environmental samples that were positive for Legionella, meaning that this pathogen was present in the water provided by the city [138]. This study suggests that UV irradiation may be an effective way of preventing pathogens from entering a premise plumbing system [138]. However, UV lamps do not create any type of residual, so they cannot influence systems that are already well-colonized [138].
In addition to not providing a residual, the current technology of mercury lamps that is used for UV irradiation has several shortcomings [139]. The most pressing concern is that improperly disposed mercury lamps are hazardous to both the environment and public health [139]. They are also not energy efficient because of their relatively low wall-plug efficiency, which is between 15% and 35% [139]. Mercury lamps also have a short lifetime of around 10,000 hours [139]. Due to these shortcomings, UV lamps are not often used as a disinfection technology [139].
4.2. UV Light Emitting Diodes (LEDs)
While low-pressure (LP) mercury lamps are an effective way to treat water known to contain Legionella, they have a number of drawbacks [139]. The emerging technology of LEDs, however, has several advantages over mercury lamps [139]. One of the biggest advantages of LEDs over LP mercury lamps is their ability to emit at targeted wavelengths [79]. LP mercury lamps emit at 254 nm, while LEDs can emit at many different wavelengths in the UV-B and UV-C [30]. Irradiating at specific wavelengths allows LEDs to target particular components of a cell [30]. The maximum absorbance of nucleic acids is around 260 nm, while proteins have a relative maximum absorbance of around 280 nm [30]. Targeting one of the components may result in greater efficacy of inactivation. Furthermore, Legionella has evolved mechanisms of photoreactivation and dark-repair that repair damages to DNA [34]. However, repair enzymes and proteins are required for these mechanisms to fix the formed dimers [140]. By targeting the proteins of a cell, the ability to repair the damaged DNA may be negatively impacted [140]. Thus, the ability to emit at targeted wavelengths may allow for LEDs to have greater efficacy of inactivation when compared to low pressure mercury lamps.
LEDs also have some practical advantages over mercury lamps [30]. While LP lamps contain mercury, LEDs are made of gallium/aluminum nitride or aluminum nitride, neither of which are toxic nor hazardous to the environment [30]. LEDs are also more compact and robust than LP lamps, allowing for increased durability [31]. Additionally, LEDs can be turned on and off with high frequency, while LP lamps require time to warm up [31]. By 2020, LEDs are projected to have a longer lifetime—over 100,000 hours—and less energy consumption than LP lamps, as they are expected to operate at 75% wall plug efficiency [31]. These physical properties, and the ability to emit at different wavelengths, would allow LEDs to be more practical than LP lamps at treating waterborne pathogens [31].
Currently, few studies have analyzed whether LEDs have the same efficacy of inactivation as LP lamps. One study compared LEDs emitting at 265 nm, 280 nm, and 300 nm to an LP lamp emitting at 254 nm to determine whether the novel technology was comparatively effective at inactivating L. pneumophila [141]. The LED emitting at 265 nm outperformed the LP lamp, but the LEDs emitting at 280 nm and 300 nm had decreased efficacy compared to the LP lamp [141]. Therefore, the wavelength used seems to be a factor in whether LEDs are as effective as LP [141]. Further studies should be conducted to determine whether other wavelengths of LEDs are equally as effective as LP lamps. However, based on the current research, LEDs may be a viable alternative to the current technology.
The development and validation of a POU device that uses LEDs may be done as a future study. By creating a POU device, disinfection could occur immediately before it is used by the consumer. This would be particularly important for premise plumbing systems that are well-colonized by waterborne pathogens, as they would be inactivated right before reaching the end user. Further studies could also be performed to determine whether there is a synergistic effect between UV LEDs and other common treatment technologies, such as copper-silver ionization, chlorine, chlorine dioxide, or monochloramine. While UV irradiation is commonly thought of as a point-of-contact strategy, the addition of the aforementioned chemicals is typically used to treat systemic issues, as they have the ability to maintain residuals throughout the premise plumbing system. If a synergistic effect existed, lower doses of the chemicals may be used, resulting in the production of fewer DBPs.
4.3. Innovative Point-of-Use (POU) Filters
With an updated focus on waterborne infection control, health care facilities are now seeking guidance on proactive prevention approaches to improve water quality to meet this higher standard. This can be achieved through additional water treatment or the use of POU filters, particularly in these high-risk areas [142]. POU filters can provide a physical barrier between waterborne pathogens and susceptible individuals and play an important role in preventing LD and other waterborne infections. Several review studies indicate that POU filters are an effective approach for preventing exposure to Legionella spp [126,131]. Although carbon based POU filters were not recommended for the removal of microorganisms, carbon filters can be used as a temporary measure for remediation situations to remove waterborne pathogens. However, these filters are recognized as a critical problem associated with the disposal of the contaminated filters due to microbial clogging and bacterial regrowth on carbon filter media. In our recent study [18], electrically heatable carbon nanotube (CNT) POU filters were developed for effective removal of Legionella from water and in-situ inactivation of Legionella on membrane surfaces to overcome the microbial clogging issue using direct current power. The CNT POU filters effectively removed Legionella (>99.99%) (i.e., below detection limit) and were able to inactive them on the membrane surface at 100% efficiency within 60 s using Joule heating at 20 V [13]. The novel POU filters could be used as a final barrier to provide efficient rejection of pathogens and thereby simultaneously eliminate microorganisms in public and private water supplies.
5. Summary
As Legionella and its associated diseases continue to capture public attention, it is important to find effective ways to mitigate the risk posed by premise plumbing. There are many studies in the peer reviewed literature that demonstrate an ability to inactivate Legionella, via either chemical or physical treatment. Possible chemical options include the injection of chlorine, monochloramine, chlorine dioxide, ozonation, or copper-silver ions. While they have all demonstrated variable effectiveness with inactivating Legionella in both bench-scale experiments and real-world applications, they come with notable negative effects. These include the risks of higher corrosion rates of plumbing and adverse health effects if ingested above the maximum contaminant level. Additionally, to be effective, these chemicals must reach the distal points of the systems at the required concentrations. This can be challenging as many of these compounds degrade over time, resulting in the formation of disinfection byproducts. Physical treatments, such as thermal inactivation or media filtration, were also reported to have some successes with treating unsafe water. However, real-world applications have found them laborious and time-consuming. Thermal inactivation requires every potential outlet be flushed for extended periods of time, while filters must be changed at regular intervals to ensure they do not foul. New technologies are being developed in response to these shortcomings. UV irradiation has been used as a treatment method for several years, but not typically in premise plumbing settings due to the short lifespan of mercury lamps and its associated environmental hazards. Furthermore, while UV can successfully inactivate pathogens at the point of installation, it cannot be used as a systemic fix to a well-colonized system. The emergence of LEDs allows for a device effective at the POU. This would disinfect drinking water prior to public consumption. As Legionella and other waterborne pathogens continue to pose a public health threat, the development of novel technologies, such as LED POU devices and CNT POU filters, will be important to promote safe drinking water.
Author Contributions
Literature review, K.M.C., L.A.B., S.C., and H.R.; writing—original draft preparation, K.C.; writing—review and editing, K.M.C., L.A.B., S.C., and H.R.; supervision, S.C. and H.R.; project Administration, H.R. All authors have read and agreed to the published version of the manuscript.
Funding
The U.S. Environmental Protection Agency, through its Office of Research and Development, funded and managed the research described herein. This work was partially supported by the Ohio Water Resources Center funding (Project number: 2017OH518B).
Acknowledgments
We thank Joshua Criss for his editorial review of this manuscript. We also thank Katherine Loizos for illustration. This work was subjected to the agency’s administrative review and approved for external publication. Any opinions expressed in this paper are those of the authors and do not necessarily reflect the views of the agency; therefore, no official endorsement should be inferred. Any mention of trade names or commercial products does not constitute endorsement or recommendation for use.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Fraser, D.W.; Tsai, T.R.; Orenstein, W.; Parkin, W.E.; Beecham, H.J.; Sharrar, R.G.; Harris, J.; Mallison, G.F.; Martin, S.M.; McDade, J.E.; et al. Legionnaires’ Disease: Description of an Epidemic of Pneumonia. N. Engl. J. Med. 1978, 297, 1189–1197. [Google Scholar] [CrossRef]
- Benitez, A.J.; Winchell, J.M. Clinical Application of a Multiplex Real-Time PCR Assay for Simultaneous Detection of Legionella Species, Legionella pneumophila, and Legionella pneumophila Serogroup 1. J. Clin. Microbiol. 2013, 51, 348–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerbel, W.; Krause, J.D.; Shelton, B.G.; Springston, J. (Eds.) Recognition, Evaluation, and Control of Legionella in Building Water Systems; American Industrial Hygiene Association: Falls Church, VA, USA, 2015. [Google Scholar]
- Centers for Disease Control and Prevention. Developing a Water Management Program to Reduce Legionella Growth and Spread in Buildings: A Practical Guide to Implementing Industry Standards. 2016. Available online: https://www.cdc.gov/Legionella/WMPtoolkit (accessed on 5 June 2017).
- New York City Department of Health. Title 10, Part 4 of the Official Compilation of Codes, Rules and Regulations of the State of New York, 2016. 2016. Available online: https://www.health.ny.gov/regulations/nycrr/title_10 (accessed on 24 February 2020).
- Centers for Medicaid and Medicare Services. Requirement to Reduce Legionella Risk in Healthcare Facility Water Systems to Prevent Cases and Outbreaks of Legionnaires’ Disease (LD); US Department of Health and Human Services, Centers for Medicaid and Medicare services, Center for Clinical Standards and Quality/Survey and Certification Group: Baltimore, MD, USA, 2017. Available online: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/Policy-and-Memos-to-States-and-Regions.html (accessed on 24 February 2020).
- American Society of Heating, Refrigerating and Air-Conditioning Engineers. Legionellosis: Risk Management for Building Water Systems. ANSI/ASHRAE Standard 188. Atlanta: The Society. 2018. Available online: https://www.ashrae.org/technical-resources/bookstore/ansi-ashrae-standard-188-2018-legionellosis-risk-management-for-building-water-systems (accessed on 24 February 2020).
- Marston, B.J.; Plouffe, J.F.; File, T.M.; Hackman, B.A.; Salstrom, S.J.; Lipman, H.B.; Kolczak, M.S.; Breiman, R.F. Incidence of Community-Acquired Pneumonia Requiring Hospitalization. Arch. Intern. Med. 1997, 157, 1709–1718. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Outbreak Reporting System (NORS). 2017. Available online: https://wwwn.cdc.gov/norsdashboard/ (accessed on 24 February 2020).
- Collier, S.A.; Stockman, L.J.; Hicks, L.A.; Garrison, L.E.; Zhou, F.J.; Beach, M.J. Direct Healthcare Costs of Selected Diseases Primarily or Partially Transmitted by Water. Epidemiol. Infect. 2012, 140, 2003–2013. [Google Scholar] [CrossRef] [Green Version]
- Beauté, J. European Legionnaires’ Disease Surveillance Network. Legionnaires’ Disease in Europe, 2011 to 2015. Eurosurveillance 2017, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Communicable Diseases Network Australia. Australia’s Notifiable Disease Status, 2014: Annual Report of the National Notifiable Disease Surveillance System. J. Commun. Dis. 2016, 40, E48–E145. [Google Scholar]
- Oh, Y.; Noga, R.; Shanov, V.; Ryu, H.; Chandra, H.; Yadav, B.; Yadav, J.; Chae, S. Electrically heatable carbon nanotube point-of-use filters for effective separation and in-situ inactivation of Legionella pneumophila. Chem. Eng. J. 2019, 366, 21–26. [Google Scholar] [CrossRef]
- Haley, C.E.; Cohen, M.L.; Halter, J.; Meyer, R.D. Nosocomial Legionnaires’ Disease: A Continuing Common-Source Epidemic at Wadsworth Medical Center. Ann. Intern. Med. 1979, 90, 583–586. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Epidemiologic Notes and Reports: Legionnaires’ Disease Outbreak Associated with a Grocery Store Mist Machine-Louisiana, 1989. Morb. Mortal. Wkly. Rep. 1990, 39, 108–110. [Google Scholar]
- Fenstersheib, M.D.; Miller, M.; Diggins, C.; Liska, S.; Detwiler, L.; Werner, S.B.; Lindquist, D.; Thacker, W.L.; Benson, R.F. Outbreak of Pontiac Fever due to Legionella anisa. Lancet 1990, 336, 35–37. [Google Scholar] [CrossRef]
- Jernigan, D.B.; Hofman, J.; Cetron, M.S.; Genese, C.A.; Nuorti, J.P.; Fields, B.S.; Benson, R.F.; Carter, R.J.; Edelstein, P.H.; Guerrero, I.C.; et al. Outbreak of Legionnaires’ Disease Among Cruise Ship Passengers Exposed to a Contaminated Whirlpool Spa. Lancet 1996, 347, 494–499. [Google Scholar] [CrossRef]
- Van Heijnsbergen, E.; Schalk, J.A.C.; Euser, S.M.; Brandsema, P.S.; de Boer, J.W.; de Roda Husman, A.M. Confirmed and Potential Sources of Legionella Reviewed. Environ. Sci. Technol. 2015, 49, 4797–4815. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.A.; Hamilton, M.T.; Johnson, W.; Jjemba, P.; Bukhari, Z.; LeChevallier, M.; Haas, C.N.; Gurian, P.L. Risk-Based Critical Concentrations of Legionella pneumophila for Indoor Residential Water Uses. Environ. Sci. Technol. 2019, 53, 4528–4541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United States Environmental Protection Agency. Technologies for Legionella Control in Premise Plumbing Systems: Scientific Literature Review; USEPA: Washington, DC, USA, 2016.
- Kirmeyer, G.; Martel, K.; Thompson, G.; Radder, L.; Klement, W.; LeChevallier, M.; Baribeau, H.; Flores, A. Optimizing Chloramine Treatment; Water Research Foundation and AWWA: Denver, CO, USA, 2004. [Google Scholar]
- United States Environmental Protection Agency (USEPA). National Primary Drinking Water Regulations: Stage 2 Disinfectants and Disinfection Byproducts Rule; Final Rule; 71 FR 388. (January 4, 2006); USEPA: Washington, DC, USA, 2006.
- Sarver, E.; Dodson, K.; Scardina, R.P.; Lattyak-Slabaugh, R.; Edwards, M.; Nguyen, C. Copper Pitting in Chlorinated, High-pH Potable Water. J. AWWA 2011, 103, 86–97. [Google Scholar] [CrossRef]
- World Health Organization. Drinking Water Guidelines, 4th ed.; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Rohr, U.; Senger, M.; Selenka, F.; Turley, R.; Wilhelm, M. Four Years of Experience with Silver-Copper Ionization for Control of Legionella in a German University Hospital Hot Water Plumbing System. Clin. Infect. Dis. 1999, 29, 1507–1511. [Google Scholar] [CrossRef]
- Araya, M.; Olivares, M.; Pizarro, F.; Llanos, A.; Figueroa, G.; Uauy, R. Community-based Randomized Double-blind Study of Gastrointestinal Effects and Copper Exposure in Drinking Water. Environ. Health Perspect. 2004, 112, 1068–1073. [Google Scholar] [CrossRef]
- Hong, J.H.; Duncan, S.E.; Dietrich, A.M. Effect of Copper Speciation at Different pH on Temporal Sensory Attributes of Copper. Food Qual. Prefer. 2010, 21, 132–139. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. Ultraviolet Disinfection Guidance Manual for the Final Long Term 2 Enhanced Surface Water Treatment Rule; USEPA: Washington, DC, USA, 2006.
- Wright, H.; Gaithuma, D.; Heath, M.; Schulz, C.; Bogan, T.; Cabaj, A.; Schmalweiser, A.; Schmelzer, M.; Finegan-Kelly, J. UV Disinfection Knowledge Base; Water Research Foundation: Denver, CO, USA, 2012. [Google Scholar]
- Vilhunen, S.; Sarkka, J.; Silanpaa, M. Ultraviolet Light-Emitting Diodes in Water Disinfection. Environ. Sci. Pollut. Res. 2009, 16, 439–442. [Google Scholar] [CrossRef]
- Wurtele, M.A.; Kolbe, T.; Lipsz, M.; Kulberg, A.; Weyers, M.; Kneissl, M.; Jekel, M. Application of GaN-based Ultraviolet-C Light Emitting Diodes—UV LEDs—For Water Disinfection. Water Res. 2011, 45, 1481–1489. [Google Scholar] [CrossRef]
- Cameron, D.C.; Grant, M. Institutional Outbreak of Pneumonia. Morb. Mortal. Wkly. Rep. 1965, 14, 265–266. [Google Scholar]
- Glick, T.H.; Gregg, M.B.; Berman, B.; Mallison, G.; Rhodes, W.W.; Kassanoff, I. Pontiac Fever: An Epidemic of Unknown Etiology in a Health Department. Am. J. Epidemiol. 1978, 107, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, A.F.; McDade, J.E.; Patton, C.M.; Bennett, J.V.; Skaliy, P.; Feeley, J.C.; Anderson, D.C.; Potter, M.E.; Newhouse, V.F.; Gregg, M.B.; et al. Pontiac Fever: Isolation of the Etiologic Agent (Legionella Pneumophila) and Demonstration of its Mode of Transmission. Am. J. Epidemiol. 1981, 114, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Phin, N.; Parry-Ford, F.; Harrison, T.; Stagg, H.R.; Zhang, N.; Kumar, K.; Lortholary, O.; Sumla, A.; Abubakar, I. Epidemiology and Clinical Management of Legionnaires’ Disease. Lancet 2014, 14, 1011–1021. [Google Scholar] [CrossRef]
- Michigan Department of Health and Human Services. Legionellosis Outbreak-Genesee County, May 2015–October 2015: Full Analysis; Michigan Department of Health and Human Services: Lansing, CO, USA, 2016. [Google Scholar]
- Bellinger, D.C. Lead Contamination in Flint-An Abject Failure to Protect Public Health. N. Engl. J. Med. 2016, 324, 1101–1103. [Google Scholar] [CrossRef]
- Michigan Department of Health and Human Services. Summary of Legionellosis Outbreak-Genesee County, June 2014–March 2015; Michigan Department of Health and Human Services: Lansing, CO, USA, 2015. [Google Scholar]
- Stout, J.E.; Yu, V.L. Legionellosis. N. Engl. J. Med. 1997, 337, 682–687. [Google Scholar] [CrossRef]
- Hicks, L.A.; Garrison, L.E.; Nelson, G.E. Legionellosis-United States, 2000–2009. Morb. Mortal. Wkly. Rep. 2011, 60, 1083–1086. [Google Scholar]
- Koo, D.T.; Dean, A.G.; Slade, R.W.; Knowles, C.M.; Adams, D.A.; Fortune, W.K.; Hall, P.A.; Fagan, R.F.; Panter-Connah, B.; Holden, H.R.; et al. MMWR Summary of Notifiable Diseases, United States, 1993. Morb. Mortal. Wkly. Rep. 1994, 42, 1–73. [Google Scholar]
- Joseph, C.A.; Ricketts, K.D.; On behalf of the European Working Group for Legionella Infections. Legionnaires’ Disease in Europe 2007–2008. Surveill. Outbreak Rep. 2010, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chandler, F.W.; Hicklin, M.D.; Blackmon, J.A. Demonstration of the Agent of Legionnaires’ Disease in Tissue. N. Engl. J. Med. 1977, 297, 1218–1220. [Google Scholar] [CrossRef]
- Friedman, S.; Spitalny, K.; Barbaree, J.; Faur, Y.; McKinney, R. Pontaic Fever Outbreak Associated with a Cooling Tower. Am. J. Public Health 1987, 77, 568–572. [Google Scholar] [CrossRef] [Green Version]
- McDade, J.E.; Shepard, C.C.; Fraser, D.W.; Tsai, T.R.; Redus, M.A.; Dowdle, W.R. Isolation of a Bacterium and Demonstration of Its Role in Other Respiratory Disease. N. Engl. J. Med. 1977, 297, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Steigerwalt, A.G.; Weaver, R.E.; McDade, J.E.; Feeley, J.C.; Mandel, M. Classification of the Legionnaires’ Disease Bacterium: An Interim Report. Curr. Microbiol. 1978, 1, 71–75. [Google Scholar] [CrossRef]
- Brenner, D.J. Deoxyribonucleic Acid Reassociation in the Taxonomy of Enteric Bacteria. Int. J. Syst. Bacteriol. 1972, 23, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Weaver, R.E. Cultural and Staining Characteristics. In Legionnaires’: The Disease, the Bacterium, and Methodology; Centers for Disease Control and Prevention: Atlanta, GA, USA, 1978; pp. 18–21. [Google Scholar]
- Diederen, B.M.W. Legionella spp. and Legionnaires’ Disease. J. Infect. 2008, 56, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Politi, B.D.; Fraser, D.W.; Mallison, G.F.; Mohatt, J.V.; Morris, G.L.; Patton, C.M.; Feeley, J.C.; Telle, R.D.; Bennett, J.V. A Major Focus of Legionnaires’ Disease in Bloomington, Indiana. Ann. Intern. Med. 1979, 90, 587–591. [Google Scholar] [CrossRef]
- Brown, A.; Yu, V.L.; Elder, E.M.; Magnussen, M.H.; Kroboth, F. Nosocomial Outbreak of Legionnaires’ Disease at the Pittsburgh Veterans Administration Medical Center. Trans. Assoc. Am. Physicians 1980, 93, 52–59. [Google Scholar]
- Conwill, D.E.; Werner, S.B.; Dritz, S.K.; Bissett, M.; Coffey, E.; Nygaard, G.; Bradford, L.; Morrison, F.R.; Knight, M.W. Legionellosis: The 1980 San Franciscan Outbreak. Am. Rev. Respir. Dis. 1982, 126, 666–669. [Google Scholar]
- Garbe, P.L.; Davis, B.J.; Weisfeld, J.S.; Markowitz, L.; Miner, P.; Garrity, F.; Barbaree, J.M.; Reingold, A.L. Nosocomial Legionnaires’ Disease: Epidemiologic Demonstration of Cooling Towers as a Source. J. Am. Med. Assoc. 1985, 254, 521–524. [Google Scholar] [CrossRef]
- Brown, C.M.; Nuorti, P.J.; Breiman, R.F.; Hathcock, A.L.; Fields, B.S.; Lipman, H.B.; Lleyellyn, G.C.; Hofman, J.; Cetron, M. A Community Outbreak of Legionnaires’ Disease Linked to Hospital Cooling Towers: An Epidemiological Method to Calculate Dose of Exposure. Int. J. Epidemiol. 1999, 28, 353–359. [Google Scholar] [CrossRef] [Green Version]
- Quinn, C.; Demirjian, A.; Watkins, L.F.; Tomczyk, S.; Lucas, C.; Brown, E.; Kozak-Muiznieks, N.; Benitez, A.; Garrison, L.E.; Kunz, J.; et al. Legionnaires’ Outbreak at a Long-Term Care Facility Caused by a Cooling Tower Using an Automated Disinfection System-Ohio, 2013. J. Environ. Health 2015, 78, 8–13. [Google Scholar]
- Hlady, W.G.; Mullen, R.C.; Mitz, C.S.; Shelton, B.G.; Hopkins, R.S.; Daikos, G.L. Outbreak of Legionnaires’ Disease Linked to a Decorative Fountain by Molecular Epidemiology. Am. J. Epidemiol. 1993, 138, 555–562. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, R.E.; Kightlinger, L.; Werpy, M.C.; Brown, E.; Stevens, V.; Hepper, C.; Keane, T.; Venson, R.F.; Fields, B.S.; Moore, M.R. Restaurant Outbreak of Legionnaires’ Disease Associated with a Decorative Fountain: An Environmental and Case-Control Study. BMC Infect. Dis. 2007, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Legionnaires’ Disease Associated with a Whirlpool Spa Display-Virginia, September-October, 1996. Morb. Mortal. Wkly. Rep. 1997, 46, 336. [Google Scholar]
- Murga, R.; Forster, T.S.; Brown, E.; Pruckler, J.M.; Fields, B.S.; Donlan, R.M. Role of Biofilms in the Survival of Legionella pneumophila in a Model Potable-Water System. Microbiology 2001, 147, 3121–3126. [Google Scholar] [CrossRef] [Green Version]
- Lau, H.Y.; Ashbolt, N.J. The Role of Biofilms and Protozoa in Legionella Pathogenesis: Implications for Drinking Water. J. Appl. Microbiol. 2008, 107, 368–378. [Google Scholar] [CrossRef]
- Declerck, P.; Behets, J.; van Hoef, V.; Ollevier, F. Detection of Legionella spp. and Some of Their Amoeba Hosts in Floating Biofilms from Anthropogenic and Natural Aquatic Environments. Water Res. 2007, 41, 3159–3167. [Google Scholar] [CrossRef]
- Declerck, P.; Behets, J.; Margineanu, A.; van Hoef, V.; Keersmaecker, B.D.; Ollevier, F. Replication of Legionella pneumophila in Biofilms of Water Distribution Pipes. Microbiol. Res. 2009, 164, 593–603. [Google Scholar] [CrossRef]
- Sabria, M.; Yu, V.L. Hospital-acquired Legionellosis: Solutions for a Preventable Solutions. Lancet Infect. Dis. 2002, 2, 368–373. [Google Scholar] [CrossRef]
- Fields, B.S.; Benson, R.F.; Besser, R.E. Legionella and Legionnaires’ Disease: 25 Years of Investigation. Clin. Microbiol. Rev. 2002, 15, 506–526. [Google Scholar] [CrossRef] [Green Version]
- Rowbotham, T.J. Preliminary Report on the Pathogenicity of Legionella pneumophila for Freshwater and Soil Amoebae. J. Clin. Pathol. 1980, 33, 1179–1183. [Google Scholar] [CrossRef] [Green Version]
- Horwitz, M.A. Phagocytosis of the Legionnaires’ Disease Bacterium (Legionella pneumophila) Occurs by a Novel Mechanism: Engulfment within a Pseudopod Coil. Cell 1984, 36, 27–33. [Google Scholar] [CrossRef]
- Rittiga, M.G.; Burmesterb, G.R.; Krauseb, A. Coiling Phagocytosis: When the Zipper James, the Cup is Deformed. Trends Microbiol. 1998, 6, 384–388. [Google Scholar] [CrossRef]
- Horwitz, M.A.; Silverstein, S.C. Legionnaires’ Disease Bacterium (Legionella pneumophila) Multiplies Intracellularly in Human Monocytes. J. Clin. Investig. 1980, 66, 441–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrne, B.; Swanson, M.S. Expression of Legionella pneumophila Virulence Traits in Response to Growth Conditions. Infect. Immun. 1998, 66, 3029–3034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiwald, M.; Helbig, J.H.; Luck, P.C. Laboratory Methods for the Diagnosis of Legionella Infections. J. Microbiol. Methods 1998, 33, 59–79. [Google Scholar] [CrossRef]
- IDEXX Laboratories. IDEXX Releases Revolutionary Water Test to Aid in the Fight Against Legionnaires’ Disease. 2016. Available online: https://www.idexx.com/en/about-idexx/news/newsroom-archive/idexx-releases-revolutionary-water-test-aid-fight-against-legionnaires-disease/ (accessed on 24 February 2020).
- Sartory, D.P.; Spies, K.; Lange, B.; Schneider, S.; Langer, B. Evaluation of Most Probable Number Method for the Enumeration of Legionella pneumophila from Potable and Related Water Samples. Lett. Appl. Microbiol. 2017, 64, 271–275. [Google Scholar] [CrossRef]
- Petrisek, R.; Hall, J. Evaluation of a Most Probable Number Method for the Enumeration of Legionella pneumophila from North American Potable and Nonpotable Water Samples. J. Water Health 2018, 16, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Yu, V.L.; Plouffe, J.F.; Pastoris, M.C.; Stout, J.E.; Schousboe, M.; Widmer, A.; Summersgill, J.; File, T.; Heath, C.M.; Paterson, D.L.; et al. Distribution of Legionella Species and Serogroups Isolated by Culture in Patients with Sporadic Community-Acquired Legionellosis: An International Collaborative Survey. J. Infect. Dis. 2002, 186, 127–128. [Google Scholar] [CrossRef] [Green Version]
- Marston, B.J.; Lipman, H.B.; Breiman, R.F. Surveillance for Legionnaires’ Disease: Risk Factors for Morbidity and Mortality. Arch. Intern. Med. 1994, 154, 2417–2422. [Google Scholar] [CrossRef]
- Plouffe, J.; Para, M.; Hackman, B.; Webster, L.; Maher, W. Nosocomial Legionnaires Disease: Difference in Attack Rates Associated with Two Strains of Legionella pneumophila Serogroup 1. In Legionella: Proceedings of the 2nd International Symposium; Thornsberry, C., Balows, A., Feeley, J.C., Jakubowski, W., Eds.; American Society for Microbiology: Washington, DC, USA, 1984. [Google Scholar]
- Cervero-Arago, S.; Rodriguez-Martinez, S.; Puertas-Bennasar, A.; Araujo, R.M. Effect of Common Drinking Water Disinfectants, Chlorine and Heat, on Free Legionella and Amoebae-Associated Legionella. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Venkobachar, C.; Iyengar, L.; Rao, A.V.S.P. Mechanism of Disinfection: Effect of Chlorine on Cell Membrane Functions. Water Res. 1977, 11, 727–729. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency (USEPA). Federal Register Notice; National Primary Drinking Water Regulations; Disinfectants and Disinfection Byproducts; Final Rule. 63 FR 69390; USEPA: Washington, DC, USA, 1998.
- Orsi, G.B.; Vitali, M.; Marinelli, L.; Ciorba, V.; Tufi, D.; Cimmuto, A.D.; Ursillo, P.; Fabiani, M.; Santis, S.D.; Protano, C.; et al. Legionella Control in the Water System of Antiquated Hospital Buildings by Shock and Continuous Hyperchlorination: 5 Years Experience. BMC Infect. Dis. 2014, 14, 394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Protection Surveillance Centre. National guidelines for the control of legionellosis in Ireland, 2009; Report of Legionnaires’ Disease Subcommittee of the Scientific Advisory Committee, Health Protection Surveillance Centre: Dublin, Ireland, 2009. [Google Scholar]
- Loret, J.F.; Robert, S.; Thomas, V.; Cooper, A.J.; McCoy, W.F.; Lévi, Y. Comparison of disinfectants for biofilm, protozoa and Legionella control. IWA J. Water Health 2005, 3, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Grosserode, M.; Wenzel, R.; Pfaller, M.; Helms, C. Continuous hyperchlorination for control of nosocomial Legionella pneumophila pneumonia: A 10-year follow-up of efficacy, environmental effects, and costs. In Legionella: Current Status and Emerging Perspectives; Barbaree, J.M., Breiman, R.F., Dufour, A.P., Eds.; American Society of Microbiology: Washington, DC, USA, 1993; pp. 226–229. [Google Scholar]
- Hassinen, J.; Lundbȁck, M.; Ifwarson, M.; Gedde, U.W. Deterioration of polyethylene pipes exposed to chlorinated water. Polym. Degrad. Stab. 2004, 84, 261–267. [Google Scholar] [CrossRef]
- McGuire, M.J. Eight revolutions in the history of U.S. drinking water disinfection. J. AWWA 2006, 98, 123–149. [Google Scholar] [CrossRef]
- Cooper, I.R.; Hanlon, G.W. Resistance of Legionella pneumophila serotype 1 biofilms to chlorine-based disinfection. J. Hosp. Infect. 2009, 74, 152–159. [Google Scholar] [CrossRef]
- Xing, X.; Wang, H.; Hu, C.; Liu, L. Effects of phosphate-enhanced ozone/biofiltration on formation of disinfection byproducts and occurrence of opportunistic pathogens in drinking water distribution systems. Water Res. 2018, 139, 168–176. [Google Scholar] [CrossRef]
- Fisher, I.; Kastl, G.; Sathasivan, A. New model of chlorine-wall reaction for simulating chlorine concentration in drinking water distribution systems. Water Res. 2017, 125, 427–437. [Google Scholar] [CrossRef]
- Storey, M.V.; Winiecka-Krusnell, J.; Ashbolt, N.J.; Stenström, T.A. The efficacy of heat and chlorine treatment against thermotolerant Acanthamoebae and Legionellae. Scand. J. Infect. Dis. 2004, 36, 656–662. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency (USEPA). Alternative Disinfectants and Oxidants Guidance Manual; EPA 815-R-99-014; USEPA: Washington, DC, USA, 1999.
- Lin, Y.E.; Stout, J.E.; Yu, V.L. Controlling Legionella in hospital drinking water: An evidence-based review of disinfection methods. Infect. Control Hosp. Epidemiol. 2011, 32, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Dupuy, M.; Mazoua, S.; Berne, F.; Bodet, C.; Garrec, N.; Herbelin, P.; Ménard-Szczebara, F.; Oberti, S.; Rodier, M.H.; Soreau, S.; et al. Efficiency of Water Disinfectants Against Legionella pneumophila and Acanthamoeba. Water Res. 2011, 45, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; McCann, C.; Hanrahan, J.; Jencson, A.; Joyce, D.; Fyffe, S.; Piescynski, S.; Hawks, R.; Stout, J.E.; Yu, V.L.; et al. Legionella Control by Chlorine Dioxide in Hospital Water Systems. Am. Water Works Assoc. J. 2009, 101, 117–127. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. National Primary Drinking Water Regulations; EPA 816-F-09-004; USEPA: Washington, DC, USA, 2009.
- Aieta, E.M.; Berg, J.D. A review of chlorine dioxide in drinking water treatment. J. AWWA 1986, 78, 62–72. [Google Scholar] [CrossRef]
- Landeen, L.K.; Yahya, M.T.; Gerba, C.P. Efficacy of copper and silver ions and reduced levels of free chlorine in inactivation of Legionella pneumophila. Appl. Environ. Microbiol. 1989, 55, 3045–3050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United States Environmental Protection Agency (USEPA). The Third Unregulated Contaminants Monitoring rule (UCMR3): Fact Sheet for Assessment Monitoring of List 1 Contaminants; EPA 815-F-12-003; USEPA: Washington, DC, USA, 2012.
- United States Environmental Protection Agency (USEPA). Economic Analysis for the Final Stage 2 Disinfectants and Disinfection Byproducts Rule; EPA 815-R-05-010; USEPA: Washington, DC, USA, 2005.
- Liu, Z.; Stout, J.E.; Tedesco, L.; Boldin, M.; Hwang, C.; Yu, V.L. Efficacy of ultraviolet light in preventing Legionella colonization of a hospital water distribution system. Water Res. 1995, 29, 2275–2280. [Google Scholar] [CrossRef]
- Herath, B.S.; Sathasivan, A. The chloramine stress induces the production of chloramine decaying proteins by microbes in biomass (biofilm). Chemosphere 2020, 124526. [Google Scholar] [CrossRef]
- Marchesi, I.; Ferranti, G.; Bargellini, A.; Marchegiano, P.; Predieri, G.; Stout, J.E.; Borella, P. Monochloramine and Chlorine Dioxide for Controlling Legionella pneumophila Contamination: Biocide Levels and Disinfection By-product Formation in Hospital Water Networks. J. Water Heatlh 2013, 11, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Selbes, M.; Beita-Sandi, W.; Kim, D.; Karanfil, T. The Role of Chloramine Species in NDMA Formation. Water Res. 2018, 140, 100–109. [Google Scholar] [CrossRef] [Green Version]
- United States Environmental Protection Agency (USEPA). Regulatory Determinations for the Third Drinking Water Contaminant Candidate List; Stakeholder Meeting; USEPA: Washington, DC, USA, 2011.
- United States Environmental Protection Agency (USEPA). Integrated Risk Information System (IRIS); N-Nitrosodimethylamine; CASRN 62-75-9; USEPA: Washington, DC, USA, 1993.
- United States Environmental Protection Agency (USEPA). Regional Screening Level (RSL). Summary Table. 2013. Available online: https://www.epa.gov/risk/regional-screening-levels-rsls-generic-tables (accessed on 24 February 2020).
- Zhang, X.; Pehkonen, S.O.; Kocherginsky, N.; Ellis, G.A. Copper corrosion in mildly alkaline water with the disinfectant monochloramine. Corros. Sci. 2002, 44, 2507–2528. [Google Scholar] [CrossRef]
- Cunliffe, D.A. Inactivation of Legionella pneumophila by monochloramine. Appl. Bacteriol. 1990, 68, 453–459. [Google Scholar] [CrossRef]
- Liu, Z.; Stout, J.E.; Tedesco, L.; Boldin, M.; Hwang, C.; Diven, W.F.; Yu, V.L. Controlled evaluation of copper-silver ionization in eradicating Legionella pneumophila from a hospital water distribution system. Infect. Dis. 1994, 169, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.E.; Vidic, R.D.; Stout, J.E.; Yu, V.L. Individual and Combined Effects of Copper and Silver Ions on Inactivation of Legionella pneumophila. Water Res. 1996, 30, 1905–1913. [Google Scholar] [CrossRef]
- Walraven, N.; Pool, W.; Chapman, C. Efficacy of Copper-Silver Ionisation in Controlling Legionella in Complex Water Distribution Systems and a Cooling Tower: Over 5 Years of Practical Experience. J. Water Process Eng. 2016, 13, 196–205. [Google Scholar] [CrossRef]
- Zevenhuizen, L.P.; Dolfing, J.; Eshuis, E.J.; Scholten-Koerselman, I.J. Inhibitory effects of copper on bacteria related to free ion concentration. Microb. Ecol. 1979, 5, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.E.; Vidic, R.D.; Stout, J.E.; Yu, V.L. Negative effect of high pH on biocidal efficacy of copper and silver ions in controlling Legionella pneumophila. Appl. Environ. Microbiol. 2002, 68, 2711–2715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, W.; Sathasivan, A.; Joll, C.; Wai, G.; Heitz, A.; Kristiana, I. Impact of NOM character on copper adsorption by trace ferric hydroxide from iron corrosion in water supply system. Chem. Eng. J. 2012, 200–202, 122–132. [Google Scholar] [CrossRef] [Green Version]
- Triantafyllidou, S.; Lytle, D.; Muhlen, C.; Swertfeger, J. Copper-silver ionization at a US hospital: Interaction of treated drinking water with plumbing materials, aesthetics and other considerations. Water Res. 2016, 102, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Andrews, S.A. Catalysis of copper corrosion products on chlorine decay and HAA formation in simulated distribution systems. Water Res. 2012, 46, 2665–2673. [Google Scholar] [CrossRef]
- Lytle, D.A.; Schock, M.R. Pitting corrosion of copper in waters with high pH and low alkalinity. J. AWWA 2008, 100, 115–129. [Google Scholar] [CrossRef]
- Rhoads, W.; Pruden, A.; Edwards, M.A. Interactive effects of corrosion, copper, and chloramines on Legionella and mycobacteria in hot water plumbing. Environ. Sci. Technol. 2017, 51, 7065–7075. [Google Scholar] [CrossRef]
- Zuma, F.; Lin, J.; Jonnalagadda, S.B. Ozone-initiated Disinfection Kinetics of Escherichia coli in Water. J. Environ. Sci. Health Part A 2009, 44, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Domingue, E.L.; Tyndall, R.L.; Mayberry, W.R.; Pancorbo, O.C. Effects of Three Oxidizing Biocides on Legionella pneumophila Serogroup 1. Appl. Environ. Microbiol. 1988, 54, 741–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc, D.S.; Carra, P.; Zanetti, G.; Francioli, P. Water Disinfection with Ozone, Copper and Silver Ions, and Temperature Increase to Control Legionella: Seven Years of Experience in a University Teaching Hospital. J. Hosp. Infect. 2005, 60, 69–72. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency (USEPA). Microbial and Disinfection Byproducts Rules Simultaneous Compliance Guidance Manual; EPA 815-R-99-015; USEPA: Washington, DC, USA, 1999.
- United States Environmental Protection Agency (USEPA). Simultaneous Compliance Guidance Manual for the Long Term 2 and Stage 2 DBP Rules; EPA 815-R-07-017; USEPA: Washington, DC, USA, 2007.
- Lee, J.; Kaletunc, G. Evaluation of the Heat Inactivation of Escherichia coli and Lactobacillus plantarum by Differential Scanning Calorimetry. Appl. Environ. Microbiol. 2002, 68, 5379–5386. [Google Scholar] [CrossRef] [Green Version]
- Chapter 29: Plumbing Systems; 2015 International Building Code; International Code Council: Washington, DC, USA, 2015.
- Mouchtouri, V.; Velonakis, E.; Hadjichristodoulou, C. Thermal Disinfection of Hotels, Hospitals, and Athletic Venues Hot Water Distribution Systems Contaminated by Legionella Species. Am. J. Infect. Control 2007, 35, 623–627. [Google Scholar] [CrossRef]
- Sheffer, P.J.; Stout, J.E.; Wagener, M.M.; Muder, R.R. Efficacy of New Point-of-Use Water Filter for Preventing Exposure to Legionella and Waterborne Bacteria. Am. J. Infect. Control 2005, 33, S20–S25. [Google Scholar] [CrossRef]
- Sharma, H. Colonization of Granular Activated Carbon Media Filters by Legionella and Heterotrophic Bacterial Cells. Master’s Thesis, Arizona State University, Tempe, AZ, USA, 2014. [Google Scholar]
- Molloy, S.L.; Ives, R.; Hoyt, A.; Taylor, R.; Rose, J.B. The use of copper and silver in carbon point-of-use filters for the suppression of Legionella throughput in domestic water systems. Appl. Microbiol. 2008, 104, 998–1007. [Google Scholar] [CrossRef]
- Daeschlein, G.; Krüger, W.H.; Selepko, C.; Rochow, M.; Dölken, G.; Kramer, A. Hygienic safety of reusable tap water filters (GermLyser®) with an operating time of 4 or 8 weeks in a haematological oncology transplant unit. BMC Infect. Dis. 2007, 7, 45. [Google Scholar] [CrossRef] [Green Version]
- Marchesi, I.; Marchegiano, P.; Bargellini, A.; Cencetti, S.; Frezza, G.; Miselli, M.; Borella, P. Effectiveness of different methods to control Legionella in the water supply: Ten-year experience in an Italian university hospital. Hosp. Infect. 2011, 77, 47–51. [Google Scholar] [CrossRef]
- Baron, J.L.; Peters, T.; Shafer, R.; MacMurray, B.; Stout, J.E. Field evaluation of a new point-of-use faucet filter for preventing exposure to Legionella and other waterborne pathogens in health care facilities. Am. J. Infect. Control 2014, 42, 1193–1196. [Google Scholar] [CrossRef]
- States, S.; Kuchta, J.; Young, W.; Conley, L.; Ge, J.; Costeloa, M.; Dowling, J.; Wadowsky, R. Controlling Legionella using copper-silver ionization. J. AWWA 1998, 90, 122–129. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Silver in drinking water: Background document for development of WHO Guidelines for Drinking-water Quality; WHO/SDE/WSH/03.04/14; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Bernard, B.; Gate, G. Epidemic of Obscure Illness- Pontiac, Michigan. Morb. Mortal. Wkly. Rep. 1968, 17, 315–320. [Google Scholar]
- Knudson, G.B. Photoreactivation of UV-Irradiated Legionella pneumophila and Other Legionella Species. Appl. Environ. Microbiol. 1985, 49, 975–980. [Google Scholar] [CrossRef] [Green Version]
- Oguma, K.; Katayama, J.; Mitani, H.; Morita, S.; Hirata, T.; Ohgaki, S. Determination of Pyrimidine Dimers in Escherichia coli and Cryptosporidium parvum During UV Light Inactivation, Photoreactivation, and Dark Repair. Appl. Environ. Microbiol. 2001, 67, 4630–4637. [Google Scholar] [CrossRef] [Green Version]
- Franzin, L.; Cabodi, D.; Fantino, C. Evaluation of the efficacy of ultraviolet irradiation for disinfection of hospital water contaminated by Legionella. Hosp. Infect. 2002, 51, 269. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.K.; Giannetta, E.T.; Getchell-White, S.E.; Durbin, L.J.; Farr, B.M. Ultraviolet Light Disinfection of Hospital Water for Preventing Nosocomial Legionella Infection: A 13-Year Follow-Up. Infect. Control Hosp. Epidemiol. 2003, 24, 580–583. [Google Scholar] [CrossRef]
- Song, K.; Mohseni, M.; Taghipour, F. Application of Ultraviolet Light-Emitting Diodes (UV-LEDs) for Water Disinfection: A Review. Water Res. 2016, 94, 341–349. [Google Scholar] [CrossRef]
- Chevremont, A.C.; Farnet, A.M.; Coulomb, B.; Boudenne, J.L. Effect of Coupled UV-A and UV-C LEDs on Both Microbiological and Chemical Pollution of Urban Wastewaters. Sci. Total Environ. 2012, 426, 304–310. [Google Scholar] [CrossRef]
- Rattanakul, S.; Oguma, K. Inactivation Kinetics and Efficiencies of UV-LEDs against Pseudomonas aerginosa, Legionella pneumophila, and Surrogate Microoragnisms. Water Res. 2018, 130, 31–37. [Google Scholar] [CrossRef]
- Parkinson, J.; Baron, J.L.; Hall, B.; Bos, H.; Racine, P.; Wagener, M.M.; Stout, J.E. Point-of-use filters for prevention of health care–acquired Legionnaires’ disease: Field evaluation of a new filter product and literature review. Am. J. Infect. Control 2019. [Google Scholar] [CrossRef]
Figure 1.
Common source of Legionella transmission.

Figure 2.
Current treatment technologies for control of Legionella in premise plumbing systems.


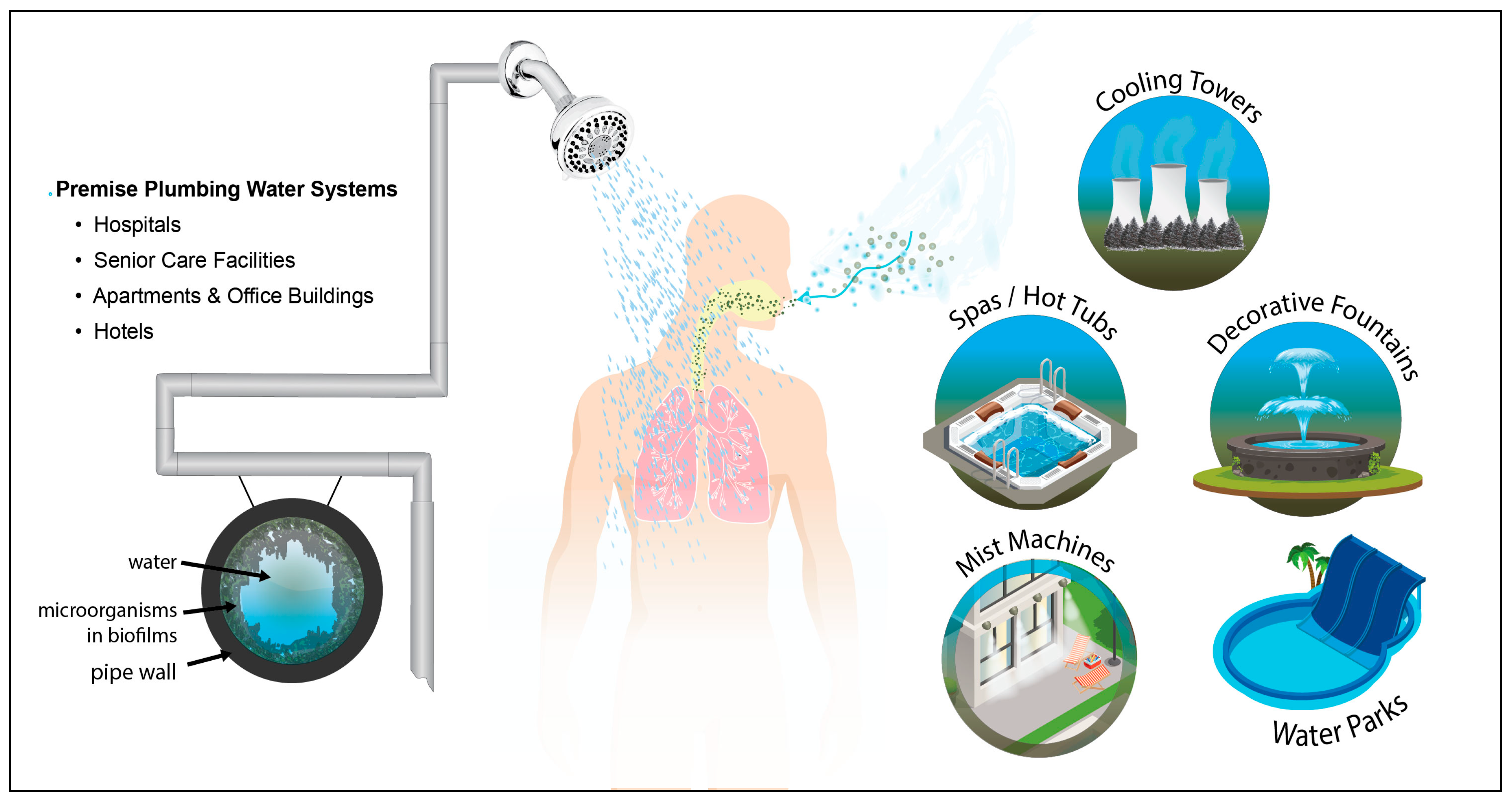{kind=link}
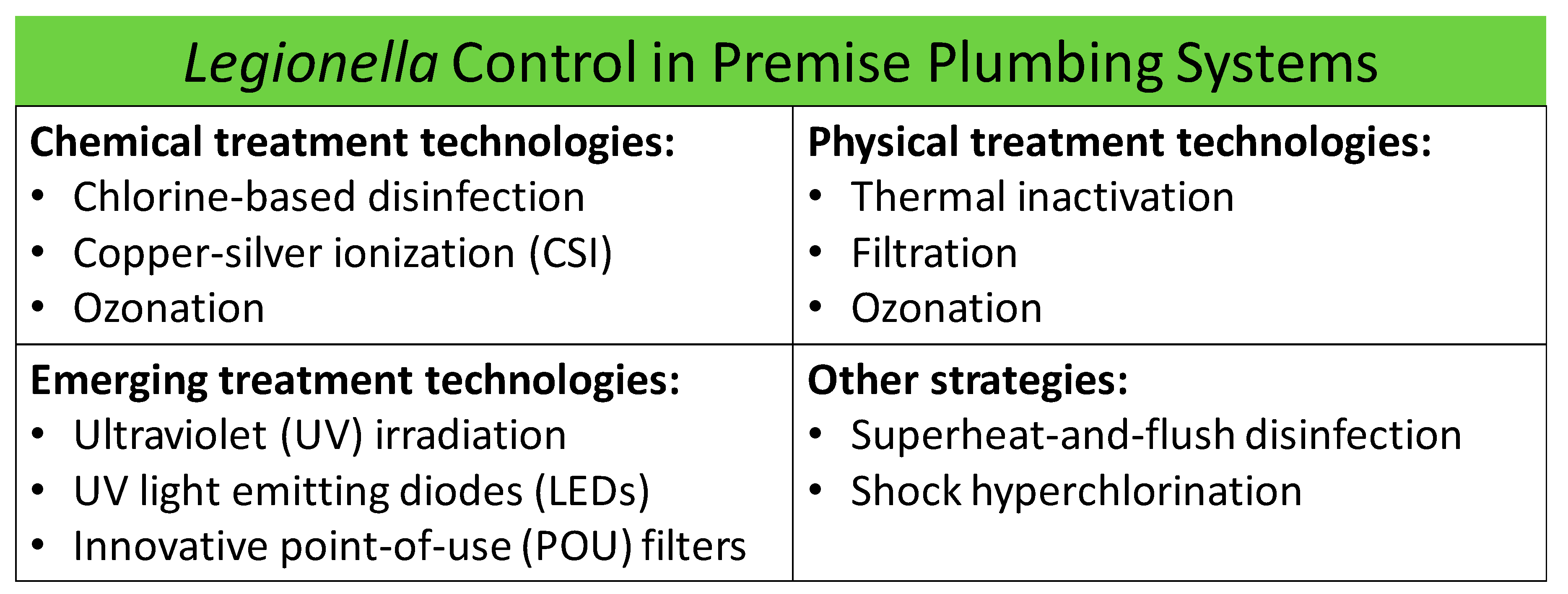{kind=link}
Table 1.
Time to 4-log reduction of various Legionella strains at two different concentrations of free chlorine. Adapted from [77].
Table 1.
Time to 4-log reduction of various Legionella strains at two different concentrations of free chlorine. Adapted from [77].
| Legionella Strains * | Time to 4-Log Reduction (Min.) | |
|---|---|---|
| 0.2 mg/L Free Chlorine | 0.5 mg/L Free Chlorine | |
| L. pneumophila serogroup 1 lab strain | Not achieved | 8 |
| L. pneumophila serogroup 1 environmental strain | Not achieved | 4 |
| L. pneumophila serogroup 7 lab strain | 9 | 2 |
| L. pneumophila serogroup 8 environmental strain | 20 | 3 |
| L. longbeachae lab strain | 11 | 3 |
* Lab strains: serogroup 1 (ATCC 33152), serogroup 7 (ATCC 33823), L. longbeachae (ATCC 33462).
Table 2.
Comparison of Legionella positivity before and after chlorination. Adapted from [80].
Table 2.
Comparison of Legionella positivity before and after chlorination. Adapted from [80].
| Condition | Number of Positive Legionella Sites (%) | Number of Negative Legionella Sites (%) | p-Value |
|---|---|---|---|
| Before chlorination | 43 (21.1) | 161 (78.9) | <0.001 |
| With continuous hyperchlorination | 23 (5.5) | 393 (94.5) |
Table 3.
Positive Legionella samples after monochloramine treatment. Adapted from [101].
Table 3.
Positive Legionella samples after monochloramine treatment. Adapted from [101].
| Treatment | Positive Samples | |
|---|---|---|
| Before Treatment | After Treatment | |
| Monochloramine System | ||
| - positive N (%) | 22/22 (100%) | 8/84 (9.5%) |
| - mean CFU/L (range) | 2.2 × 104 (1.0 × 102 – 9.5 × 105) | 3.3 × 102 (25 – 4.9 × 103) |
| Control Sytem | ||
| - positive N (%) | 84/85 (98.8%) | |
| - mean CFU/L (range) | 1.0 × 104 (25 – 1.3 × 106) | |
Table 4.
Ozone inactivation of L. pneumophila serogroup 1 at different parameters. Adapted from [119].
Table 4.
Ozone inactivation of L. pneumophila serogroup 1 at different parameters. Adapted from [119].
| Different Parameters for Inactivation of Legionella Pneumophila Serogroup 1 | |||
|---|---|---|---|
| pH | Temperature (°C) | Ozone Concentration (µg/mL) * | Log Inactivation |
| 7.2 | 25 | 0.21 | 2.37 |
| 7.2 | 35 | 0.13 | 2.21 |
| 7.2 | 45 | 0.13 | 2.55 |
| 8.0 | 25 | 0.20 | 2.45 |
| 8.9 | 25 | 0.14 | 3.28 |
* Mean concentration for the contact time of 5 min.
Table 5.
Comparison of positivity before and after ozonation in a premise plumbing system. Adapted from Blanc et al. [120].
Table 5.
Comparison of positivity before and after ozonation in a premise plumbing system. Adapted from Blanc et al. [120].
| Percent Positivity | CFU/mL | p-Value | |
|---|---|---|---|
| Before ozonation | (66/100) 66% | 10.9 ± 17 | 0.12 |
| After ozonation | (67/120) 56% | 5.2 ± 9.7 |
Table 6.
Amount of time to 4-log reduction in various Legionella strains at different temperatures. Adapted from [77].
Table 6.
Amount of time to 4-log reduction in various Legionella strains at different temperatures. Adapted from [77].
| Legionella Strain * | Time to 4-Log Reduction (Min) | ||||
|---|---|---|---|---|---|
| 50 °C/R2 | 55 °C/R2 | 60 °C/R2 | 65 °C/R2 | 70 °C/R2 | |
| L. pneumophila serogroup 1 lab strain | 117/0.80 | 10/0.92 | 2/0.90 | 0.8/0.88 | 0.9/0.79 |
| L. pneumophila serogroup 1 environmental strain | 46/0.84 | 8/0.98 | 3/0.83 | 1.4/0.90 | 0.6/0.82 |
| L. pneumophila serogroup 7 lab strain | 40/0.97 | 25/0.96 | 3/0.76 | 0.6/0.87 | 1.2/0.77 |
| L. pneumophila serogroup 8 environmental strain | 68/0.97 | 16/0.89 | 4/0.94 | 0.8/0.90 | 0.7/0.99 |
| L. longbeachae lab strain | 15/0.94 | 2/0.88 | Not achieved | Not achieved | Not achieved |
* Lab strains: serogroup 1 (ATCC 33152), serogroup 7 (ATCC 33823), L. longbeachae (ATCC 33462).
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Carlson, K.M.; Boczek, L.A.; Chae, S.; Ryu, H. Legionellosis and Recent Advances in Technologies for Legionella Control in Premise Plumbing Systems: A Review. Water 2020, 12, 676. https://doi.org/10.3390/w12030676
AMA Style
Carlson KM, Boczek LA, Chae S, Ryu H. Legionellosis and Recent Advances in Technologies for Legionella Control in Premise Plumbing Systems: A Review. Water. 2020; 12(3):676. https://doi.org/10.3390/w12030676
Chicago/Turabian StyleCarlson, Kelsie M., Laura A. Boczek, Soryong Chae, and Hodon Ryu. 2020. "Legionellosis and Recent Advances in Technologies for Legionella Control in Premise Plumbing Systems: A Review" Water 12, no. 3: 676. https://doi.org/10.3390/w12030676
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.