
Insulin-like Growth Factor 1 (IGF1), IGF Binding Protein-3 (IGFBP3) and Growth Response to Daily Zinc Supplementation: A Randomized Trial in Rural Laotian Children
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Ethical Approval
2.2. Study Design and Participants
2.3. Sample Size Considerations
2.4. Inclusion and Exclusion Criteria
2.5. Randomization
2.6. Study Interventions and Follow-Up
2.7. Data Collection
2.8. Patient and Public Involvement
2.9. Laboratory Analyses
2.10. Data Entry and Analyses
2.11. Definitions
2.12. Statistical Analyses
3. Results
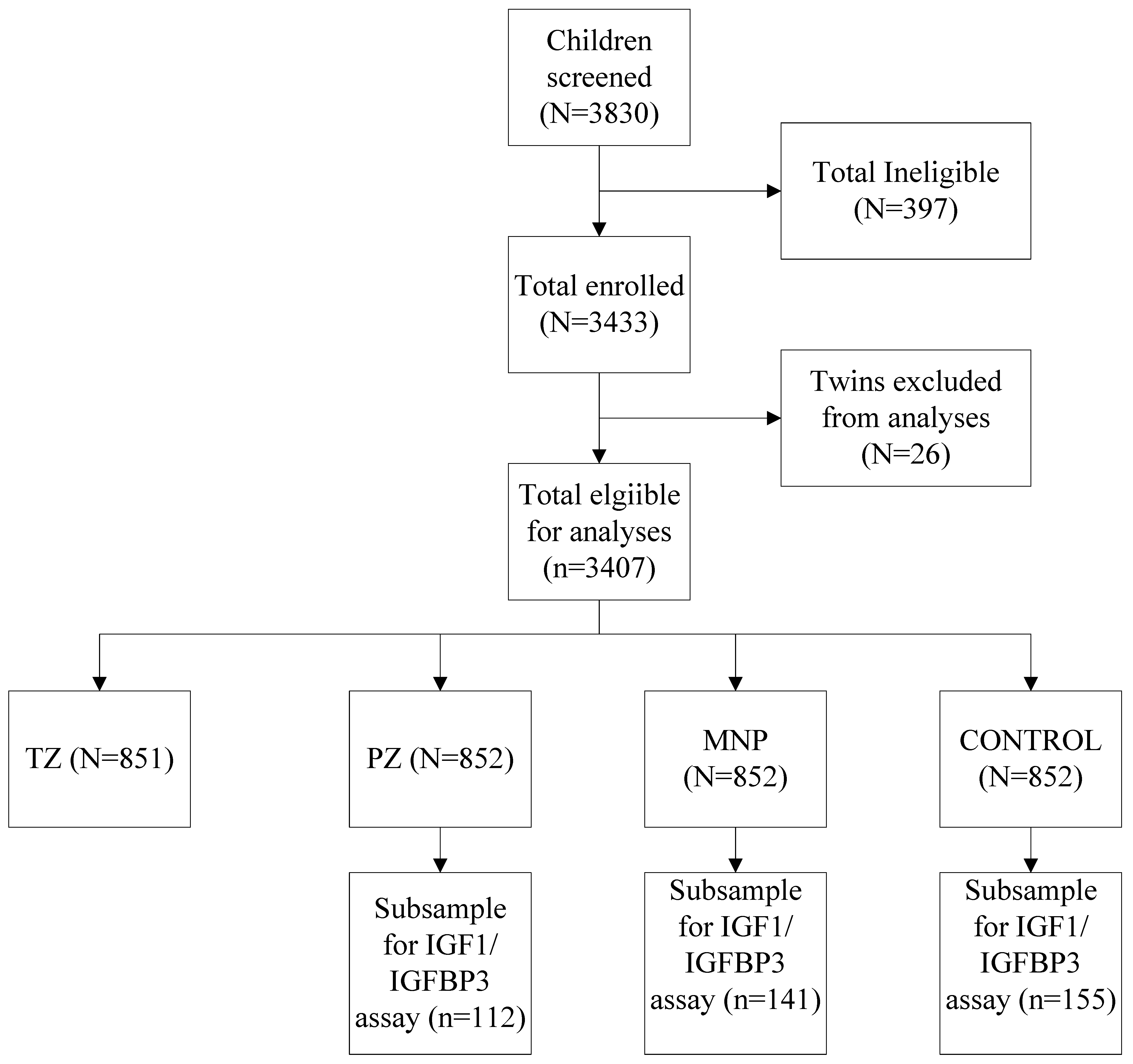
3.1. Sampling and Baseline Data
3.2. Main Effects of PZ and MNP on IGF1 and IGFBP3
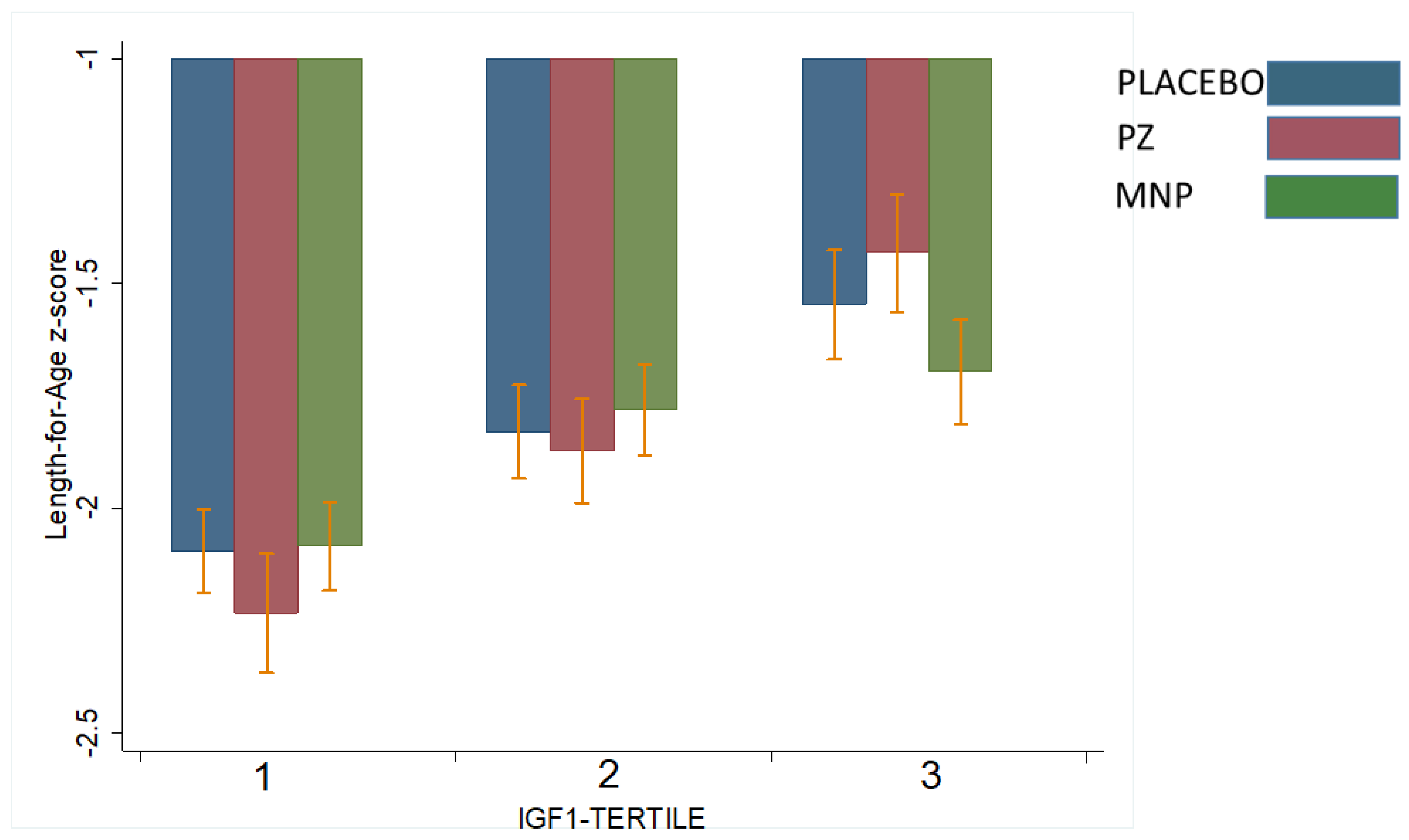
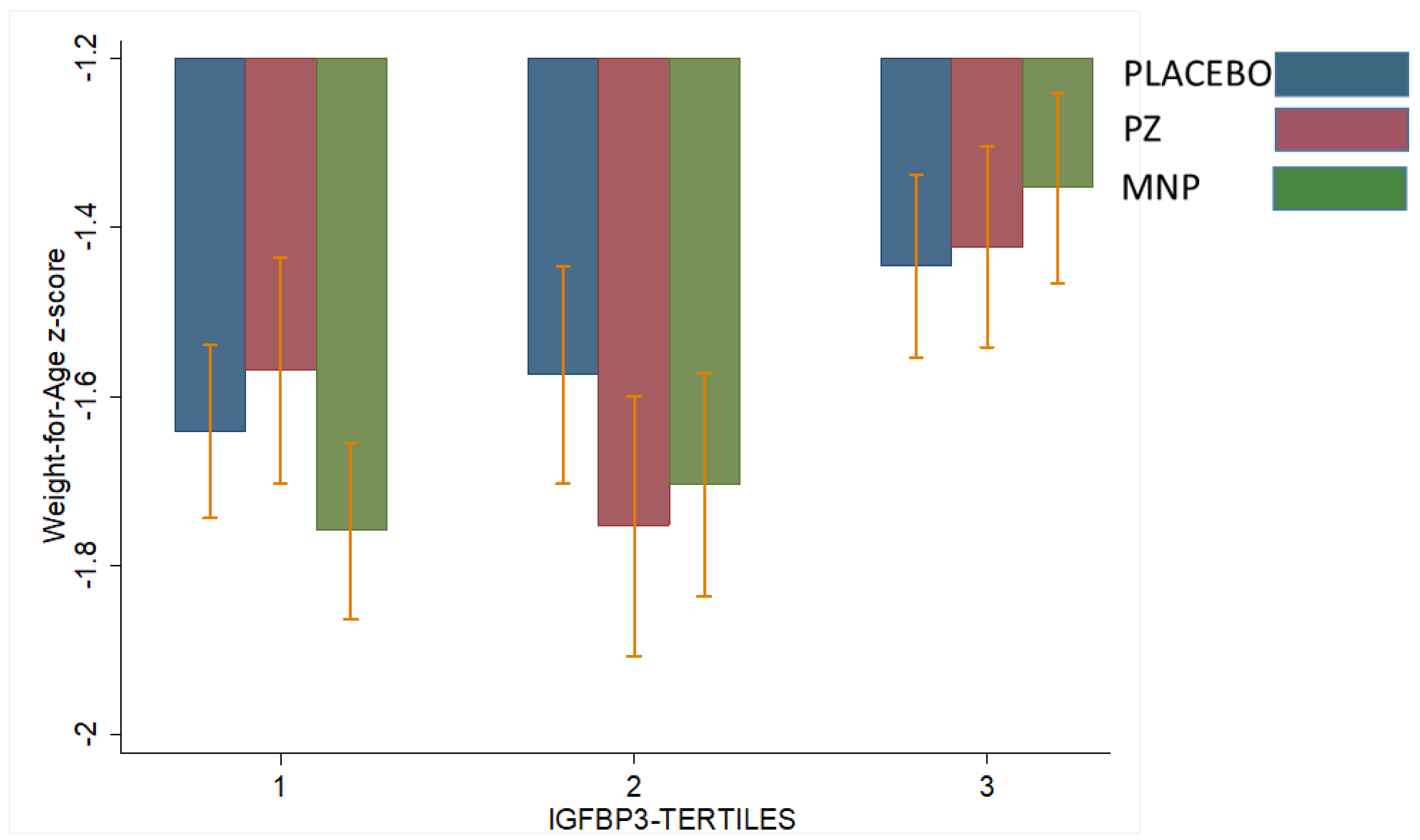
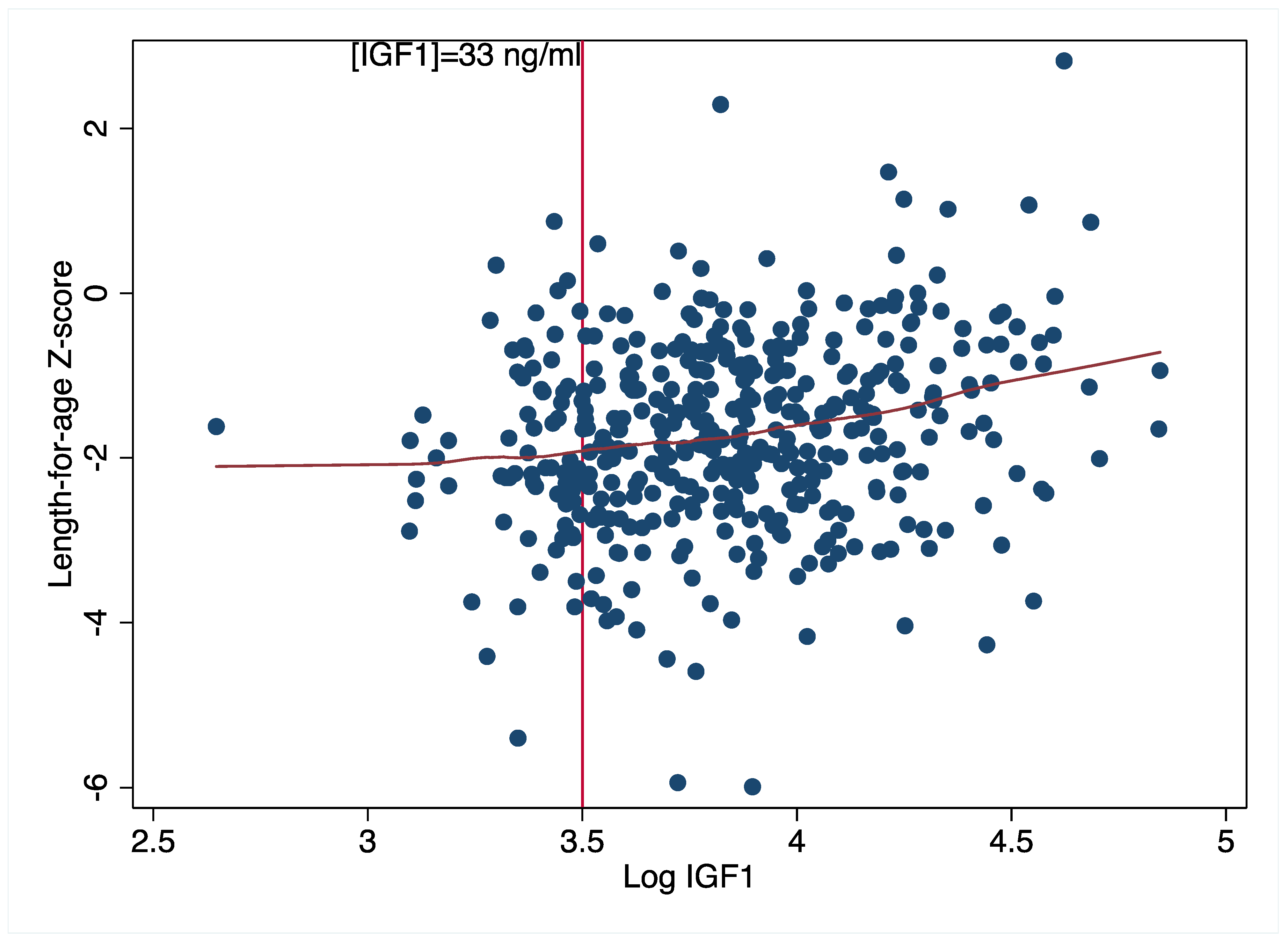
3.3. Modifying Effect of Baseline IGF1 and IGFPB3 on LAZ and WAZ
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Cousins, R.J. Metal elements and gene expression. Annu. Rev. Nutr. 1994, 14, 449–469. [Google Scholar] [CrossRef] [PubMed]
- Imdad, A.; Bhutta, Z.A. Effect of preventive zinc supplementation on linear growth in children under 5 years of age in developing countries: A meta-analysis of studies for input to the lives saved tool. BMC Public Health 2011, 11, S22. [Google Scholar] [CrossRef] [PubMed]
- Mayo-Wilson, E.; Junior, J.A.; Imdad, A.; Dean, S.; Chan, X.H.S.; Chan, E.S.; Jaswal, A.; Bhutta, Z.A. Zinc supplementation for preventing mortality, morbidity, and growth failure in children aged 6 months to 12 years of age. Cochrane Database Syst. Rev. 2014, 5, CD009384. [Google Scholar] [CrossRef]
- Brown, K.H.; Peerson, J.M.; Baker, S.K.; Hess, S. Preventive Zinc Supplementation among Infants, Preschoolers, and Older Prepubertal Children. Food Nutr. Bull. 2009, 30, S12–S40. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Peerson, J.M.; Rivera, J.; Allen, L.H. Effect of supplemental zinc on the growth and serum zinc concentrations of prepubertal children: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2002, 75, 1062–1071. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention (CDC); United Nations Children Fund (UNICEF). Global Assessment of Home Fortification Interventions, 2011; Home Fortification Technical Advisory Group: Geneva, Switzerland, 2013.
- Ramakrishnan, U.; Nguyen, P.; Martorell, R. Effects of micronutrients on growth of children under 5 y of age: Meta-analyses of single and multiple nutrient interventions. Am. J. Clin. Nutr. 2009, 89, 191–203. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Suchdev, P.S.; Vist, G.E.; Walleser, S.; Peña-Rosas, J.P. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age. Cochrane Database Syst. Rev. 2011, 1, CD008959. [Google Scholar] [CrossRef]
- Mayo-Wilson, E.; Imdad, A.; Junior, J.; Dean, S.; Bhutta, Z.A. Preventive zinc supplementation for children, and the effect of additional iron: A systematic review and meta-analysis. BMJ Open 2014, 4, e004647. [Google Scholar] [CrossRef]
- Raiten, D.J.; Raghavan, R.; Kraemer, K. Biomarkers in growth. Ann. Nutr. Metab. 2013, 63, 293–297. [Google Scholar] [CrossRef]
- Davidson, M.B. Effect of growth hormone on carbohydrate and lipid metabolism. Endocr. Rev. 1987, 8, 115–131. [Google Scholar] [CrossRef] [PubMed]
- Talwar, G.; Pandian, M.; Kumar, N.; Hanjan, S.; Saxena, R.; Krishnaraj, R.; Gupta, S. Mechanism of Action of Pituitary Growth Hormone. Recent Prog. Horm. Res. 1975, 31, 141–174. [Google Scholar] [CrossRef]
- Slootweg, M.; Van Buul-Offers, S.; Herrmann-Erlee, M.; Van Der Meer, J.; Duursma, S. Growth Hormone Is Mitogenic for Fetal Mouse Osteoblasts but Not for Undifferentiated Bone Cells. J. Endocrinol. 1988, 116, R11–R13. [Google Scholar] [CrossRef]
- Denis, I.; Pointillart, A.; Lieberherr, M. Effects of growth hormone and insulin-like growth factor-I on the proliferation and differentiation of cultured pig bone cells and rat calvaria cells. Growth Regul. 1994, 4, 123–130. [Google Scholar]
- Giustina, A.; Mazziotti, G.; Canalis, E. Growth hormone, insulin-like growth factors, and the skeleton. Endocr. Rev. 2008, 29, 535–559. [Google Scholar] [CrossRef] [PubMed]
- Spagnoli, A.; Rosenfeld, R.G. The mechanisms by which growth hormone brings about growth. The relative contributions of growth hormone and insulin-like growth factors. Endocrinol. Metab. Clin. North Am. 1996, 25, 615–631. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.; Isgaard, J.; Lindahl, A.; Dahlström, A.; Skottner, A.; Isaksson, O.G.P. Regulation by Growth Hormone of Number of Chondrocytes Containing IGF-I in Rat Growth Plate. Science 1986, 233, 571–574. [Google Scholar] [CrossRef]
- Butler, A.A.; Le Roith, D. Control of Growth by the Somatropic Axis: Growth Hormone and the Insulin-Like Growth Factors Have Related and Independent Roles. Annu. Rev. Physiol. 2001, 63, 141–164. [Google Scholar] [CrossRef] [PubMed]
- Yakar, S.; Rosen, C.J.; Beamer, W.G.; Ackert-Bicknell, C.L.; Wu, Y.; Liu, J.L.; Ooi, G.T.; Setser, J.; Frystyk, J.; Boisclair, Y.R.; et al. Circulating levels of IGF-1 directly regulate bone growth and density. J. Clin. Investig. 2002, 110, 771–781. [Google Scholar] [CrossRef]
- Ranke, M.B. Insulin-like growth factor binding-protein-3 (IGFBP-3). Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 701–711. [Google Scholar] [CrossRef]
- Doherty, C.P.; Crofton, P.M.; Sarkar, M.A.K.; Shakur, M.S.; Wade, J.C.; Kelnar, C.J.H.; Elmlinger, M.W.; Ranke, M.B.; Cutting, W.A. Malnutrition, zinc supplementation and catch-up growth: Changes in insulin-like growth factor I, its binding proteins, bone formation and collagen turnover. Clin. Endocrinol. 2002, 57, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Ninh, N.X.; Thissen, J.P.; Collette, L.; Gerard, G.; Khoi, H.H.; Ketelslegers, J.M. Zinc supplementation increases growth and circulating insulin-like growth factor I (IGF-I) in growth-retarded Vietnamese children. Am. J. Clin. Nutr. 1996, 63, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Barffour, M.A.; Hinnouho, G.-M.; Kounnavong, S.; Wessells, K.R.; Ratsavong, K.; Bounheuang, B.; Chanhthavong, B.; Sitthideth, D.; Sengnam, K.; Arnold, C.D.; et al. Effects of Daily Zinc, Daily Multiple Micronutrient Powder, or Therapeutic Zinc Supplementation for Diarrhea Prevention on Physical Growth, Anemia, and Micronutrient Status in Rural Laotian Children: A Randomized Controlled Trial. J. Pediatr. 2019, 207, 80–89.e2. [Google Scholar] [CrossRef] [PubMed]
- Barffour, M.A.; Hinnouho, G.-M.; Wessells, K.R.; Kounnavong, S.; Ratsavong, K.; Sitthideth, D.; Bounheuang, B.; Sengnam, K.; Chanhthavong, B.; Arnold, C.D.; et al. Effects of therapeutic zinc supplementation for diarrhea and two preventive zinc supplementation regimens on the incidence and duration of diarrhea and acute respiratory tract infections in rural Laotian children: A randomized controlled trial. J. Glob. Health 2020, 10, 010424. [Google Scholar] [CrossRef] [PubMed]
- Wessells, K.R.; Brown, K.H.; Kounnavong, S.; Barffour, M.A.; Hinnouho, G.-M.; Sayasone, S.; Stephensen, C.B.; Ratsavong, K.; Larson, C.P.; Arnold, C.D.; et al. Comparison of two forms of daily preventive zinc supplementation versus therapeutic zinc supplementation for diarrhea on young children’s physical growth and risk of infection: Study design and rationale for a randomized controlled trial. BMC Nutr. 2018, 4, 39. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Lao Statistics Bureau. Lao People’s Democratic Republic Special -V. Lao Social Indicator Survey (MICS/DHS) Final Report (English). Available online: https://dhsprogram.com/publications/publication-fr356-other-final-reports.cfm2012 (accessed on 30 March 2023).
- Leroy, J.L.; Ruel, M.; Habicht, J.-P.; Frongillo, E.A. Using height-for-age differences (HAD) instead of height-for-age z-scores (HAZ) for the meaningful measurement of population-level catch-up in linear growth in children less than 5 years of age. BMC Pediatr. 2015, 15, 145. [Google Scholar] [CrossRef] [PubMed]
- Hess, S.; Hinnouho, B.M.; Lao, G.M. Zinc Study Statistical Analyses Plan. 2017. Available online: https://osf.io/5bq9c/ (accessed on 26 April 2019).
- McDonald, C.M.; Suchdev, P.S.; Krebs, N.F.; Hess, S.Y.; Wessells, K.R.; Ismaily, S.; Rahman, S.; Wieringa, F.T.; Williams, A.M.; Brown, K.H.; et al. Adjusting plasma or serum zinc concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2020, 111, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.C.; Guyatt, G.H. Best (but oft-forgotten) practices: Intention-to-treat, treatment adherence, and missing participant outcome data in the nutrition literature. Am. J. Clin. Nutr. 2016, 104, 1197–1201. [Google Scholar] [CrossRef] [PubMed]
- Rocha, D.D.M.; De Brito, N.J.N.; Dantas, D.M.R.; Silva, A.D.A.; Almeida, M.D.G.; Brandão-Neto, J. Effect of Zinc Supplementation on GH, IGF1, IGFBP3, OCN, and ALP in Non-Zinc-Deficient Children. J. Am. Coll. Nutr. 2015, 34, 290–299. [Google Scholar] [CrossRef]
- Esamai, F.; Liechty, E.; Ikemeri, J.; Westcott, J.; Kemp, J.; Culbertson, D.; Miller, L.V.; Hambidge, K.M.; Krebs, N.F. Zinc Absorption from Micronutrient Powder Is Low but Is not Affected by Iron in Kenyan Infants. Nutrients 2014, 6, 5636–5651. [Google Scholar] [CrossRef]
- Alves, C.X.; Vale, S.; Dantas, M.M.G.; Maia, A.A.; Franca, M.C.; Marchini, J.S.; Leite, L.D.; Brandao-Neto, J. Positive effects of zinc supplementation on growth, GH, IGF1, and IGFBP3 in eutrophic children. J. Pediatr. Endocrinol. Metab. 2012, 25, 881–887. [Google Scholar] [CrossRef]
- Yüksel, B.; Özbek, M.N.; Mungan, N.; Darendeliler, F.; Budan, B.; Bideci, A.; Çetinkaya, E.; Berberoglu, M.; Evliyaoğlu, O.; Yeşilkaya, E.; et al. Serum IGF-1 and IGFBP-3 Levels in Healthy Children between 0 and 6 Years of Age—Original Article. J. Clin. Res. Pediatr. Endocrinol. 2011, 3, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Alberti, C.; Chevenne, D.; Mercat, I.; Josserand, E.; Armoogum-Boizeau, P.; Tichet, J.; Léger, J. Serum Concentrations of Insulin-like Growth Factor (IGF)-1 and IGF Binding Protein-3 (IGFBP-3), IGF-1/IGFBP-3 Ratio, and Markers of Bone Turnover: Reference Values for French Children and Adolescents and z-Score Comparability with Other References. Clin. Chem. 2011, 57, 1424–1435. [Google Scholar] [CrossRef]
- Hess, S.Y.; Wessells, K.R.; Hinnouho, G.-M.; Barffour, M.A.; Sanchaisuriya, K.; Arnold, C.D.; Brown, K.H.; Larson, C.P.; Fucharoen, S.; Kounnavong, S. Iron status and inherited haemoglobin disorders modify the effects of micronutrient powders on linear growth and morbidity among young Lao children in a double-blind randomised trial. Br. J. Nutr. 2019, 122, 895–909. [Google Scholar] [CrossRef]
- Kingchaiyaphum, B.; Sanchaisuriya, K.; Fucharoen, G.; Chaibunruang, A.; Hess, S.Y.; Hinnouho, G.M.; Barffour, M.A.; Wessells, K.R.; Kounnavong, S.; Fucharoen, S. Hemoglobins F, A(2), and E levels in Laotian children aged 6–23 months with Hb E disorders: Effect of age, sex, and thalassemia types. Int. J. Lab. Hematol. 2020, 42, 277–283. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis, V.; Soliman, A.; Elsedfy, H.; Skordis, N.; Kattamis, C.; Angastiniotis, M.; Karimi, M.; Yassin, M.A.D.M.; El Awwa, A.; Stoeva, I.; et al. Growth and endocrine disorders in thalassemia: The international network on endocrine complications in thalassemia (I-CET) position statement and guidelines. Indian J. Endocrinol. Metab. 2013, 17, 8–18. [Google Scholar] [CrossRef]
- De Sanctis, V.; Eleftheriou, A.; Malaventura, C. Prevalence of endocrine complications and short stature in patients with thalassaemia major: A multicenter study by the Thalassaemia International Federation (TIF). Pediatr. Endocrinol. Rev. 2004, 2 (Suppl. 2), 249–255. [Google Scholar]
- Moayeri, H.; Oloomi, Z. Prevalence of growth and puberty failure with respect to growth hormone and gonadotropins secretion in beta-thalassemia major. Arch. Iran. Med. 2006, 9, 329–334. [Google Scholar] [PubMed]
- Checkley, W.; Buckley, G.; Gilman, R.H.; Assis, A.M.; Guerrant, R.L.; Morris, S.S.; Mølbak, K.; Valentiner-Branth, P.; Lanata, C.F.; Black, R.E.; et al. Multi-country analysis of the effects of diarrhoea on childhood stunting. Leuk. Res. 2008, 37, 816–830. [Google Scholar] [CrossRef]
- Fujimoto, M.; Andrew, M.; Liao, L.; Zhang, D.; Yildirim, G.; Sluss, P.; Kalra, B.; Kumar, A.; Yakar, S.; Hwa, V.; et al. Low IGF-I Bioavailability Impairs Growth and Glucose Metabolism in a Mouse Model of Human PAPPA2 p.Ala1033Val Mutation. Endocrinology 2019, 160, 1363–1376. [Google Scholar] [CrossRef]
- Dewey, K.G. Reducing stunting by improving maternal, infant and young child nutrition in regions such as South Asia: Evidence, challenges and opportunities. Matern. Child Nutr. 2016, 12 (Suppl. 1), 27–38. [Google Scholar] [CrossRef] [PubMed]
- Wolf, E.; Schneider, M.R.; Zhou, R.; Fisch, T.M.; Herbach, N.; Dahlhoff, M.; Hoeflich, A. Functional consequences of IGFBP excess—Lessons from transgenic mice. Pediatr. Nephrol. 2005, 20, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Silha, J.V.; Gui, Y.; Murphy, L.J. Impaired glucose homeostasis in insulin-like growth factor-binding protein-3-transgenic mice. Am. J. Physiol. Metab. 2002, 283, E937–E945. [Google Scholar] [CrossRef] [PubMed]
- Modric, T.; Silha, J.V.; Shi, Z.; Gui, Y.; Suwanichkul, A.; Durham, S.K.; Powell, D.R.; Murphy, L.J. Phenotypic Manifestations of Insulin-Like Growth Factor-Binding Protein-3 Overexpression in Transgenic Mice*. Endocrinology 2001, 142, 1958–1967. [Google Scholar] [CrossRef] [PubMed]
- Silha, J.V.; Murphy, L.J. Minireview: Insights from Insulin-Like Growth Factor Binding Protein Transgenic Mice. Endocrinology 2002, 143, 3711–3714. [Google Scholar] [CrossRef]
- Veldhuis, J.D.; Iranmanesh, A. Physiological Regulation of the Human Growth Hormone (GH)-Insulin-Like Growth Factor Type I (IGF-I) Axis: Predominant Impact of Age, Obesity, Gonadal Function, and Sleep. Sleep 1996, 19 (Suppl. 10), S221–S224. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | PZ (n = 112) | MNP (n = 141) | Placebo (n = 155) |
|---|---|---|---|
| Mean Age (months) | 15.7 ± 5.3 | 15.7 ± 4.9 | 15.7 ± 5.3 |
| Males (%) | 55 (48.3) | 76 (52.4) | 85 (54.8%) |
| LAZ | 1.78 ± 1.03 | 1.77 ± 1.06 | 1.68 ± 1.09 |
| WAZ | 1.48 ± 1.01 | 1.46 ± 1.02 | 1.38 ± 1.00 |
| Stunting (%) | 51 (45.1) | 58 (40.0) | 50 (32.3) |
| Anemia (%) | 52 (45.6) | 70 (48.3) | 73 (47.1) |
| Zinc Deficiency * (%) | 87 (78.4) | 88 (73.3) | 95 (81.2) |
| Growth Biomarker | |||
| IGF1 | 47.6 (47.1, 53.8) | 46.8 (44.2, 49.5) | 46.1 (43.4, 48.7) |
| IGFBP3 | 2097 (1996–2257) | 2094 (2009, 2183) | 2131 (2046, 2215) |
| Molar IGF1:IGFBP3 ratio | 0.08 (0.07, 0.09) | 0.08 (0.07, 0.09) | 0.08 (0.07, 0.09) |
| PZ (n = 112) | MNP (n = 141) | Placebo (n = 155) | p-Value * | |
|---|---|---|---|---|
| IGF1 at endline, ng/mL | 39.1 (37.0, 41.2) | 39.2 (37.4, 41.0) | 39.0 (37.2, 40.8) | 0.99 |
| Change in IGF1, ng/mL | −7.7 (−10.3, −5.1) | −7.8 (−10.1, −5.6) | −8.2 (−10.3, −6.0) | 0.96 |
| IGFBP3 at endline, ng/mL | 2037.6 (1946.4, 2128.8) | 2075.5 (1995.5, 2155.5) | 2055.0 (1997.8, 2132.5) | 0.83 |
| Change in IGFBP3, ng/mL | −76.2 (−162.1, 9.6) | −3.6 (−77.8, 70.6) | −16.2 (−88.3, 55.9) | 0.42 |
| Molar IGF1:IGFBP3 at endline | 0.073 (0.069, 0.077) | 0.071 (0.068, 0.074) | 0.072 (0.068, 0.075) | 0.74 |
| Time Point/Baseline Factor | LAZ | WAZ |
|---|---|---|
| 18 weeks | ||
| IGF1 | 0.006 | 0.329 |
| IGFBP3 | 0.110 | 0.535 |
| 36 weeks | ||
| IGF1 | 0.32 | 0.96 |
| IGFBP3 | 0.38 | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barffour, M.A.; Bernstein, R.M.; Hinnouho, G.-M.; Wessells, K.R.; Arnold, C.D.; Kounnavong, S.; Hess, S.Y. Insulin-like Growth Factor 1 (IGF1), IGF Binding Protein-3 (IGFBP3) and Growth Response to Daily Zinc Supplementation: A Randomized Trial in Rural Laotian Children. Nutrients 2023, 15, 2590. https://doi.org/10.3390/nu15112590
Barffour MA, Bernstein RM, Hinnouho G-M, Wessells KR, Arnold CD, Kounnavong S, Hess SY. Insulin-like Growth Factor 1 (IGF1), IGF Binding Protein-3 (IGFBP3) and Growth Response to Daily Zinc Supplementation: A Randomized Trial in Rural Laotian Children. Nutrients. 2023; 15(11):2590. https://doi.org/10.3390/nu15112590
Chicago/Turabian StyleBarffour, Maxwell A., Robin M. Bernstein, Guy-Marino Hinnouho, K. Ryan Wessells, Charles D. Arnold, Sengchanh Kounnavong, and Sonja Y. Hess. 2023. "Insulin-like Growth Factor 1 (IGF1), IGF Binding Protein-3 (IGFBP3) and Growth Response to Daily Zinc Supplementation: A Randomized Trial in Rural Laotian Children" Nutrients 15, no. 11: 2590. https://doi.org/10.3390/nu15112590