
Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis



1
Private Practice: Churchill-laan 162hs, 1078 ER Amsterdam, The Netherlands
2
Department of Periodontology, School of Dental Medicine, Stony Brook University, Stony Brook, NY 11794-8712, USA
3
Department of Oral Surgery and Implant Dentistry, Johann Wolfgang Goethe University, 60596 Frankfurt, Germany
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(21), 10413; https://doi.org/10.3390/app112110413
Submission received: 19 September 2021
/
Revised: 27 October 2021
/
Accepted: 29 October 2021
/
Published: 5 November 2021
Abstract
:The aim of the present case report was to demonstrate the vertical gain in the posterior resorbed mandible utilizing the use of an Allograft Customized Bone Block. The case presents a 66-year-old healthy female nonsmoker who lost her right mandibular molars long time ago. In the past, she had an implant placement, which failed due to a fracture of the implant. Due to the high risk of mandibular nerve damage, the implant was left in the jaw and was completely covered with bone. Since the jaw was completely atrophic and short implants were not an option, a vertical ridge augmentation was required. This case report presents the use of an Allograft Customized Bone Block as a good option in patients with an atrophic mandible, showing no vertical bone resorption five months after placement and great osseointegration of the placed implants.
1. Introduction
Patients with a highly resorbed atrophic mandible who require implants have several treatment options. Inferior alveolar nerve lateralization is an alternative to augmentation; however, neurosensory dysfunctions, as well as mandibular fractures, may occur [1]. Short implants usually do not require simultaneous bone grafting, resulting in reduced surgery time and patient morbidity compared to bone grafting and regular implant placement in a one- or two stage approach [1]. However, when the bone volume is not sufficient for short implant placement, vertical bone augmentation needs to be considered as a serious treatment option.
With the modern CAD/CAM technology, it is possible based on a CBCT- or CT-scan to create patient specific bone blocks to rebuild lost hard tissue volumes. Virtual planning of the bone block requires advanced knowledge of both anatomical, as well as implant, considerations. This method has been able to show promising results in several case reports over the last couple of years [2,3,4,5,6,7]. Puros® Allograft Customized Bone Blocks (ACBB) have been available since 2014. They are prepared based on the multi-step Tutoplast® tissue sterilization process, which was developed in 1969 [4]. After purification of the donor material and milling in a clean environment, the block was packaged and sterilized with low-dose gamma irradiation [8].
Apart from the hard tissue grafting procedure, the appropriate soft tissue management is mandatory. The coronal advancement of the buccal flap technique described by Romanos [9], as well as coronally advanced lingual flap, are safe and predictable techniques to achieve tension-free soft tissue closure of the elevated flap without the risk of dehiscence [10]. Implants should be placed approximately after 6 months of healing time, since the allograft blocks will be integrated and remodeled by so-called “creeping substitution”, which has been shown to happen after 5 to 6 months [11,12].
A previous paper showed the bone dynamics and remodeling considerations for autogenous cortico-cancellous blocks, which can be also here taken into consideration for the use of allograft bone block materials [13].
Graft resorption during the initial healing period may be a result of the initial remodeling of the graft. Collagen-rich allogenous bone remodels relatively fast, which might be accompanied by superficial bone loss. Soft tissue management remains crucial [3].
2. Case Presentation
The 66-year-old patient was a healthy non-smoking female patient who lost her right mandibular molars for a long time. Previous implant placement was not successful, and an implant failure was present due to an implant fracture. Due to the risk of damaging the mandibular nerve, the broken implant was left in the jaw (as a “sleeping” implant), covered completely by the bone. That implant was left in the jaw, which presented a severe atrophy, with a remaining residual bone height of approximately 4 mm. Based on the height, the placement of short implants was not an option, and the patient was informed about the different grafting options, as well as the possible intraoperative and postoperative complications (Figure 1).
3. Pre-Surgical Planning
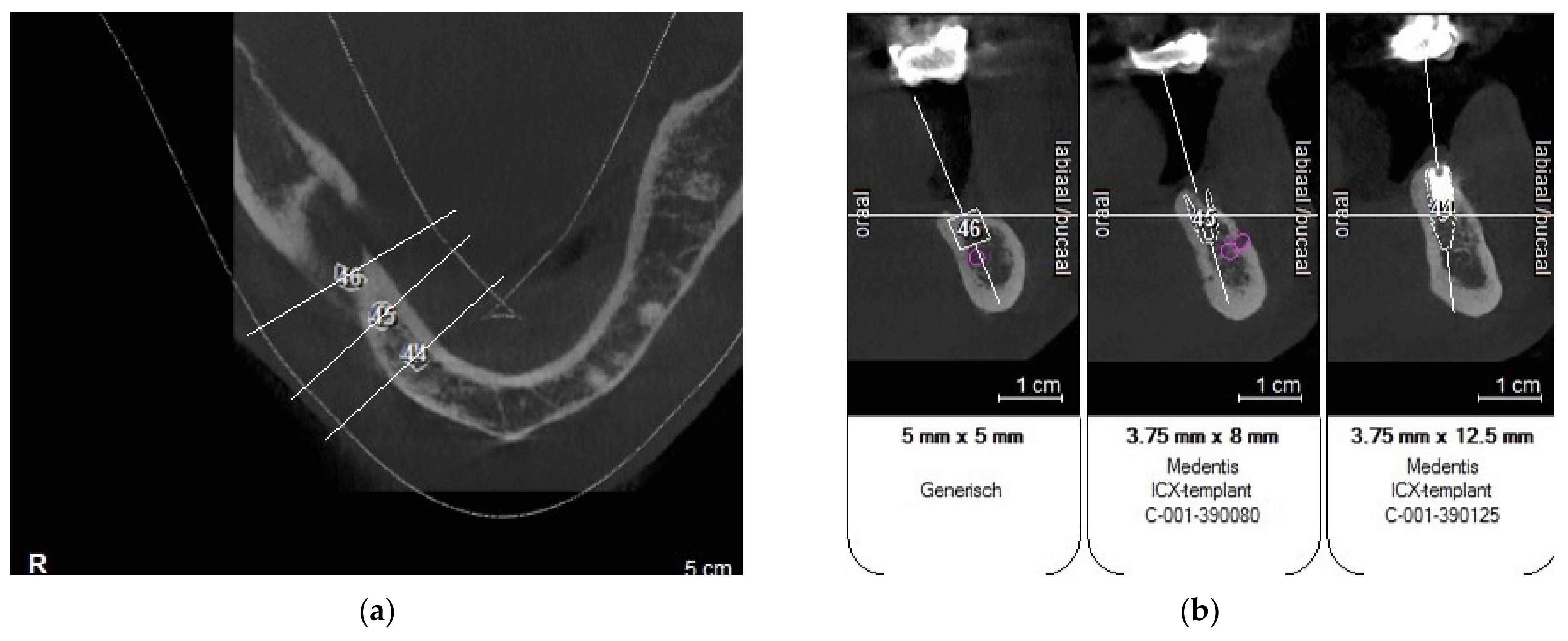
A CBCT scan was made with an initial setup for guided surgery, demonstrating a bone height less than 4 mm from the mandibular canal (Figure 2 and Figure 3a,b).
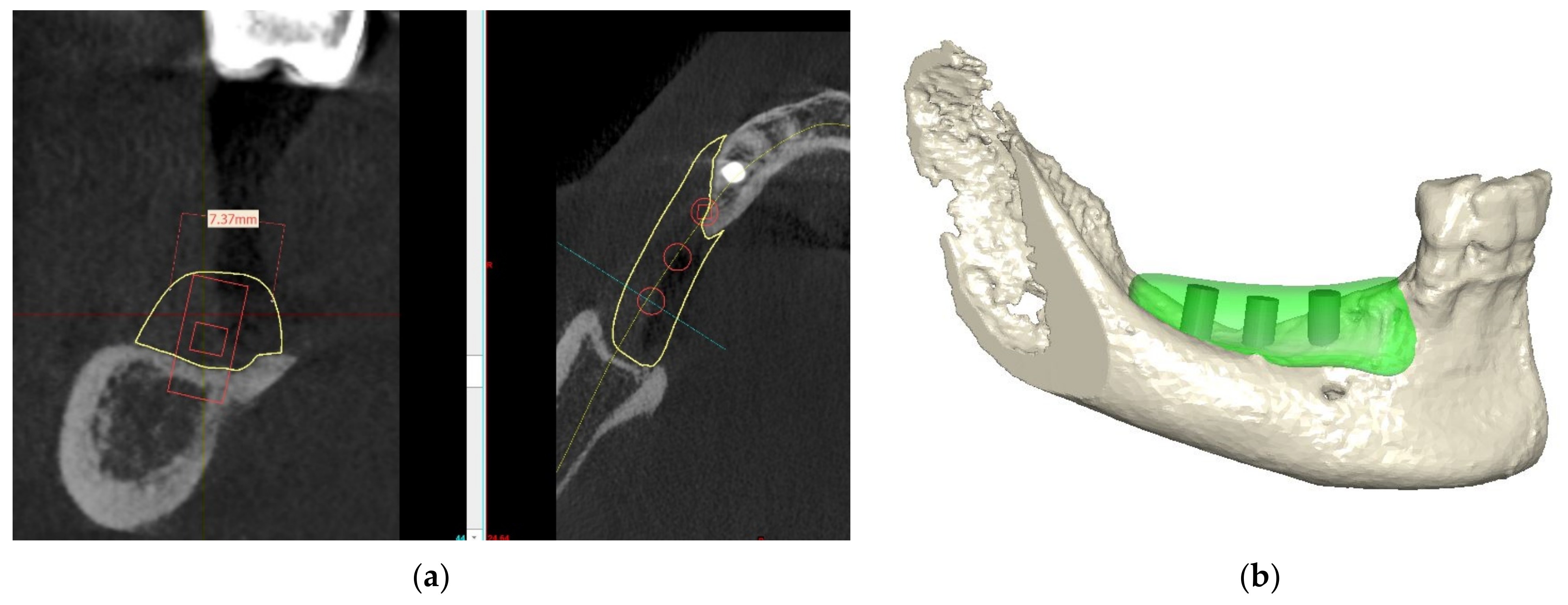
Due to the severe atrophy in the posterior mandible, different treatment options were discussed with the patient, and after agreement, informed consent was signed, including all the different potential risks and complications. The patient was extensively informed about vertical bone augmentation utilizing an allograft Customized Bone block (Puros® Allograft Customized Bone Block, Zimmer-Biomet Dental, Palm Beach Gardens, FL, USA) to reconstruct the lost hard tissue volume in the vertical and horizontal dimensions. Based on the CBCT evaluation and the implant position, the exact size of the block was determined (Figure 4a,b).
4. Materials and Methods
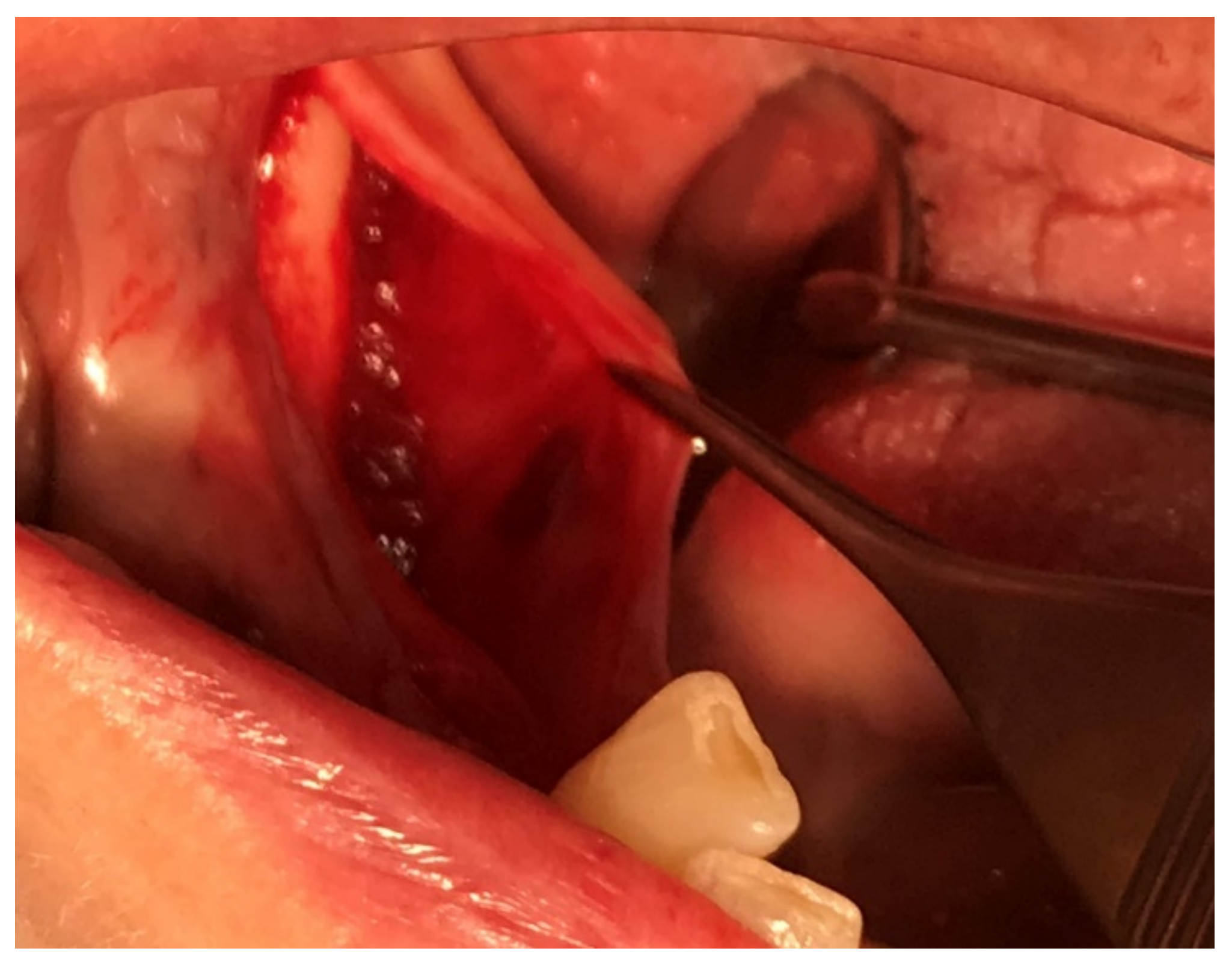
A preoperative systemic antibiotic therapy with 600 mg of clindamycin due to a history of penicillin allergy was initiated one hour before surgery, as well as supplemental pain medication with 600 mg of Ibuprofen. Chlorhexidine mouth rinse was used 60 s before surgery. Under local anesthesia with Articain (Ultracain-DS® forte), a full thickness flap elevation with a crestal incision was performed in the keratinized tissue, from the retromolar pad to the distal surface, of the most distal tooth (#27). No vertical release or elevation by the mylohyoid line was needed to get sufficient elevation of the flap (Figure 5).
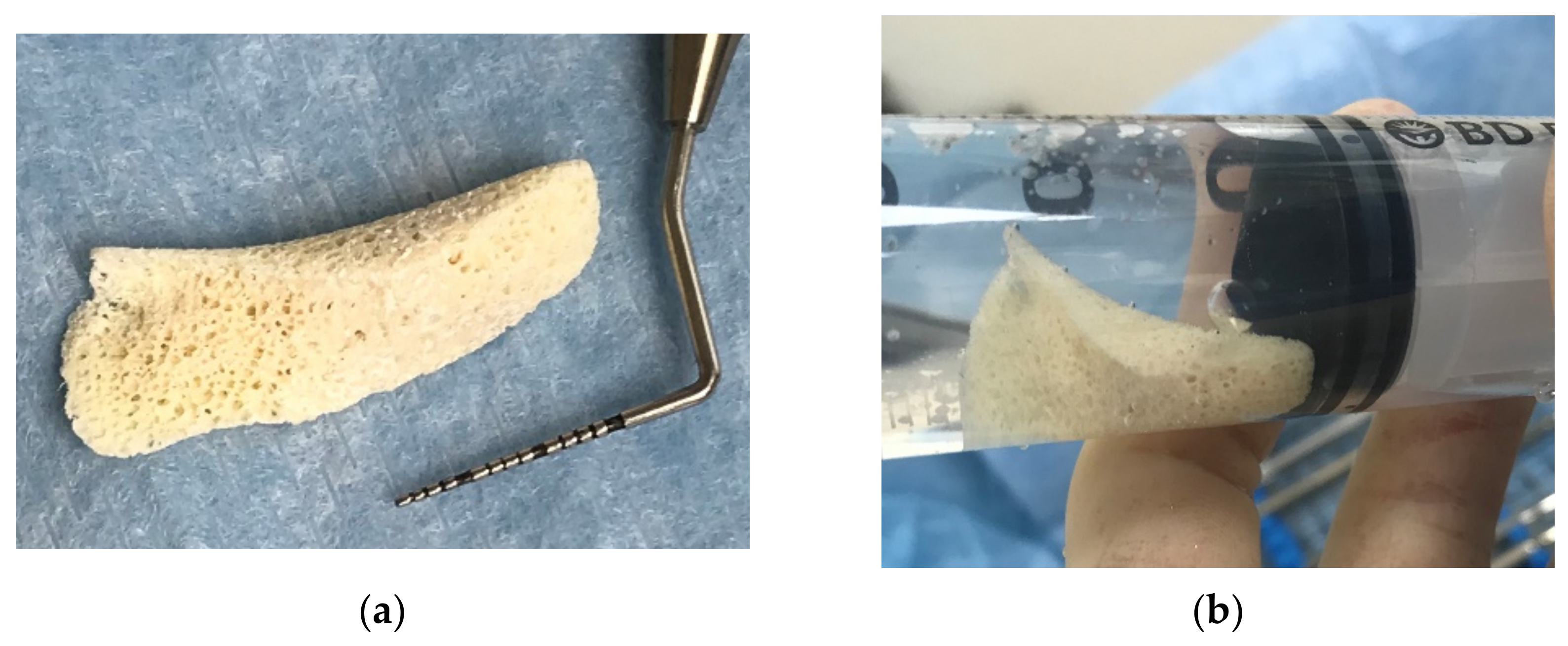
The customized bone block was rehydrated in a 0.9% sodium chloride solution according to the manufacturer’s instructions (Zimmer-Biomet Dental, Palm Beach Gardens, FL, USA) to improve the ductility and reduce the risk of fracture [14]. In order to achieve a uniform penetration of the liquid, the block was transferred into a sterile syringe with the sodium chloride solution. Special concern was made to remove all air bubbles from the block [11,15] (Figure 6a,b).
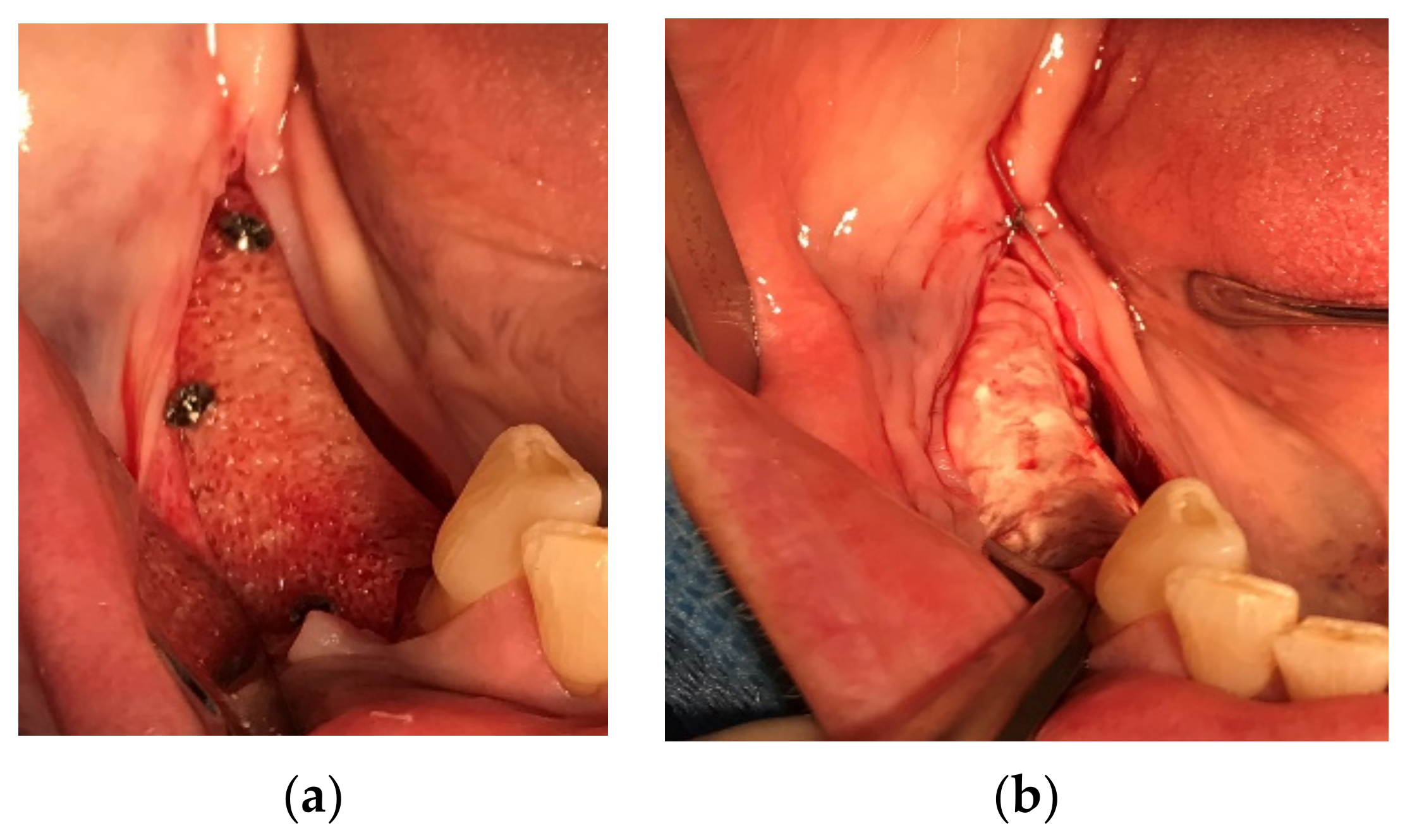
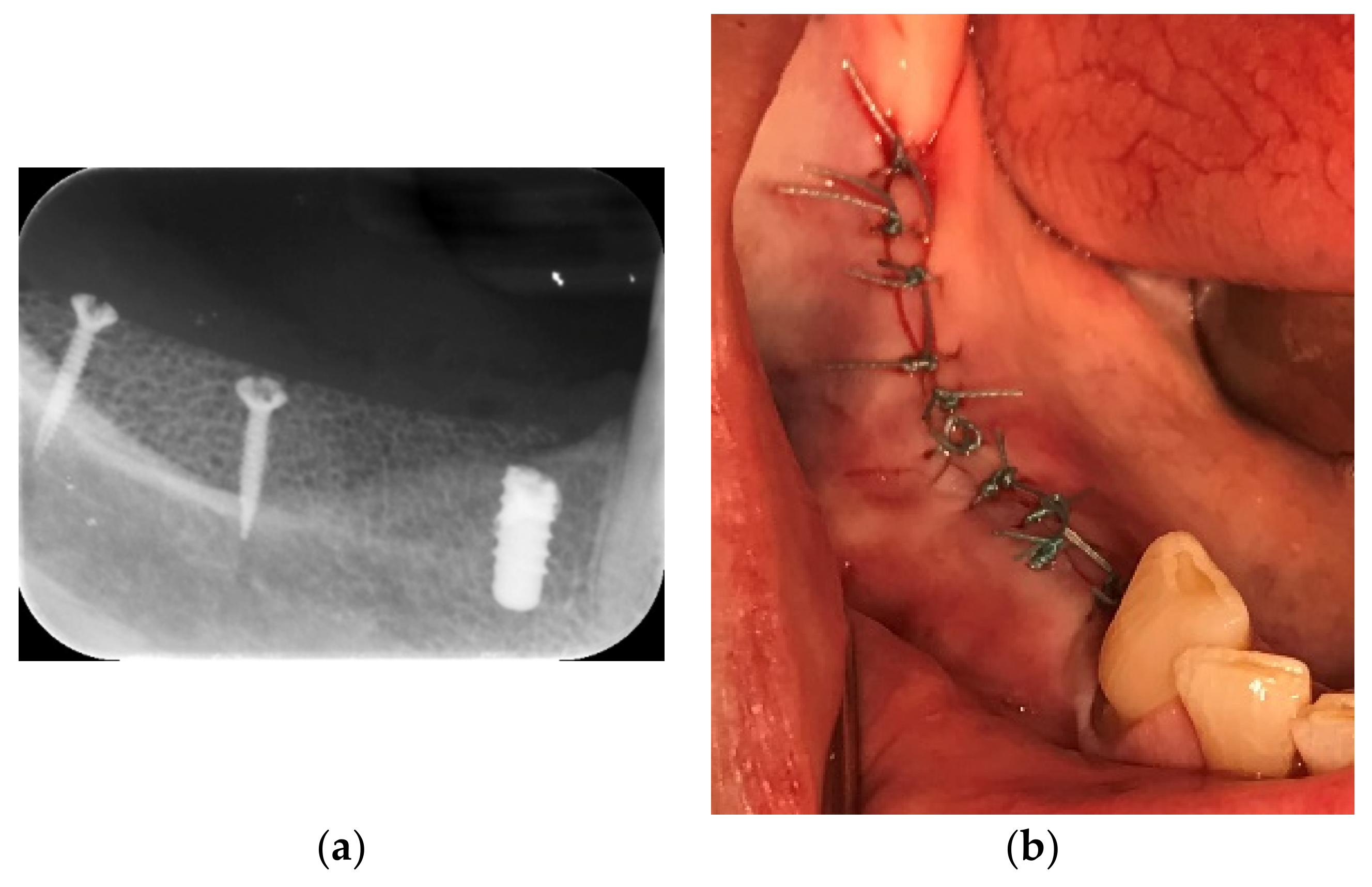
The bone block fitted precisely without a need of for adaptations. Three ACE TruFix® 1.2-mm × 6-mm screws were used to fix the block and subsequently covered with a non-crosslinked collagen membrane (CopiOs® Pericardium Membrane, Zimmer Biomet Dental). Simple interrupted sutures were applied to provide a tension-free flap closure (Figure 7a–c and Figure 8a,b). After surgery, the patient was instructed to not wear her partial prosthesis and to rinse the oral cavity with chlorhexidine solution for one minute twice a day. To prevent postoperative infection, an additional antibiotic administration with clindamycin for 5 days was prescribed (300 mg every 8 h).
5. Postoperative Case Management
Minor swelling and slight pain were observed for the first 5 days after surgery. The sutures were removed 14 days after surgery (Figure 9). Follow-up clinical examinations were performed every 4 weeks and did not present any complications.
6. Clinical Outcome
After five months, the patient was seen for a new radiological evaluation with a CBCT. The CBCT was indicated to design a surgical (prosthetic) guide for the implants to be placed. Due to this, we could superimpose and compare the designed customized bone block with the 5-month follow-up CBCT (Figure 10a,b).
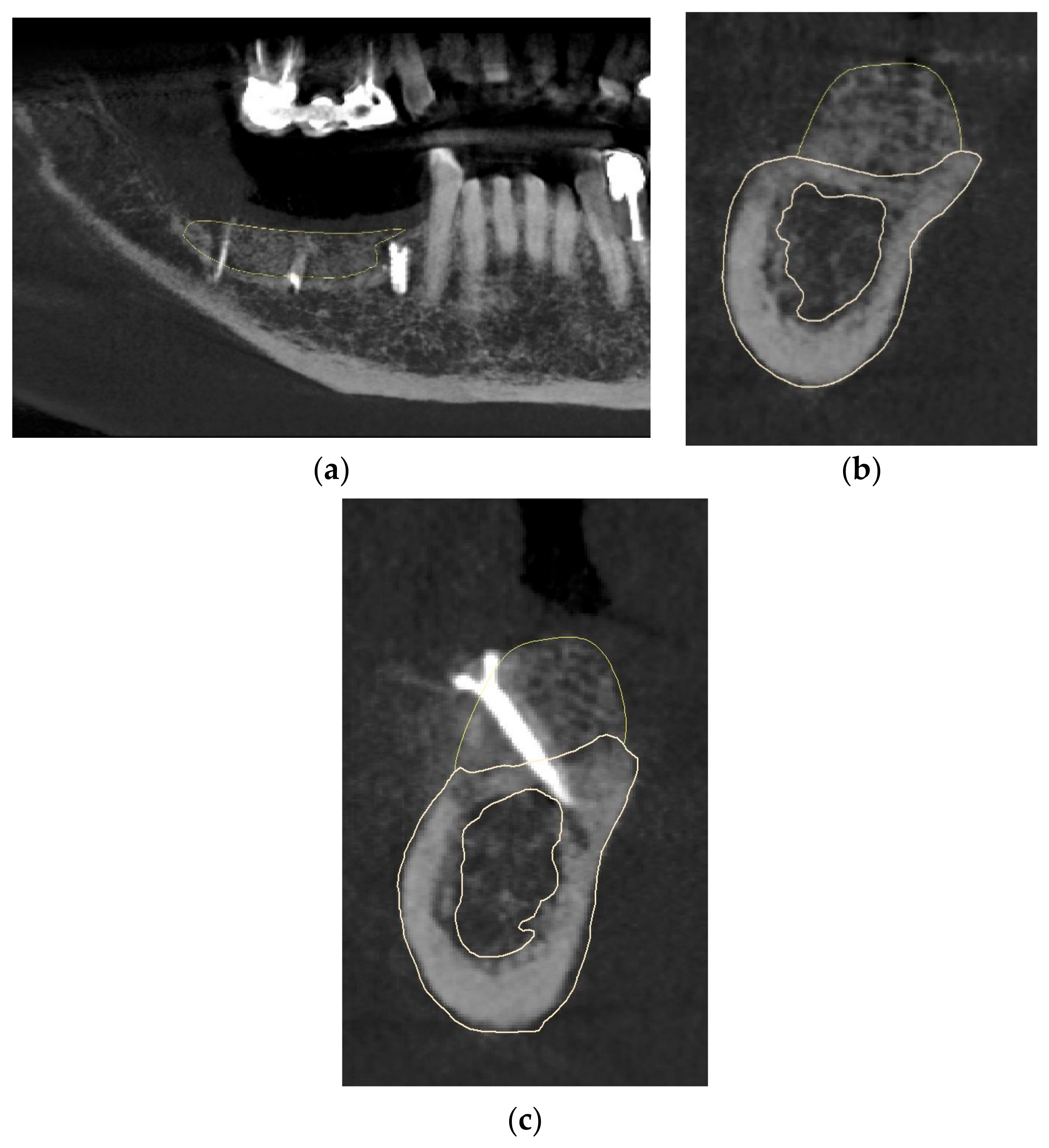
The postoperative evaluation confirmed no resorption after 5 months compared to the preoperative design of the bone block (Figure 11a). The yellow lines on the CBCT images show the design of the bone block, demonstrating no loss of volume after 5 months (Figure 11b,c).
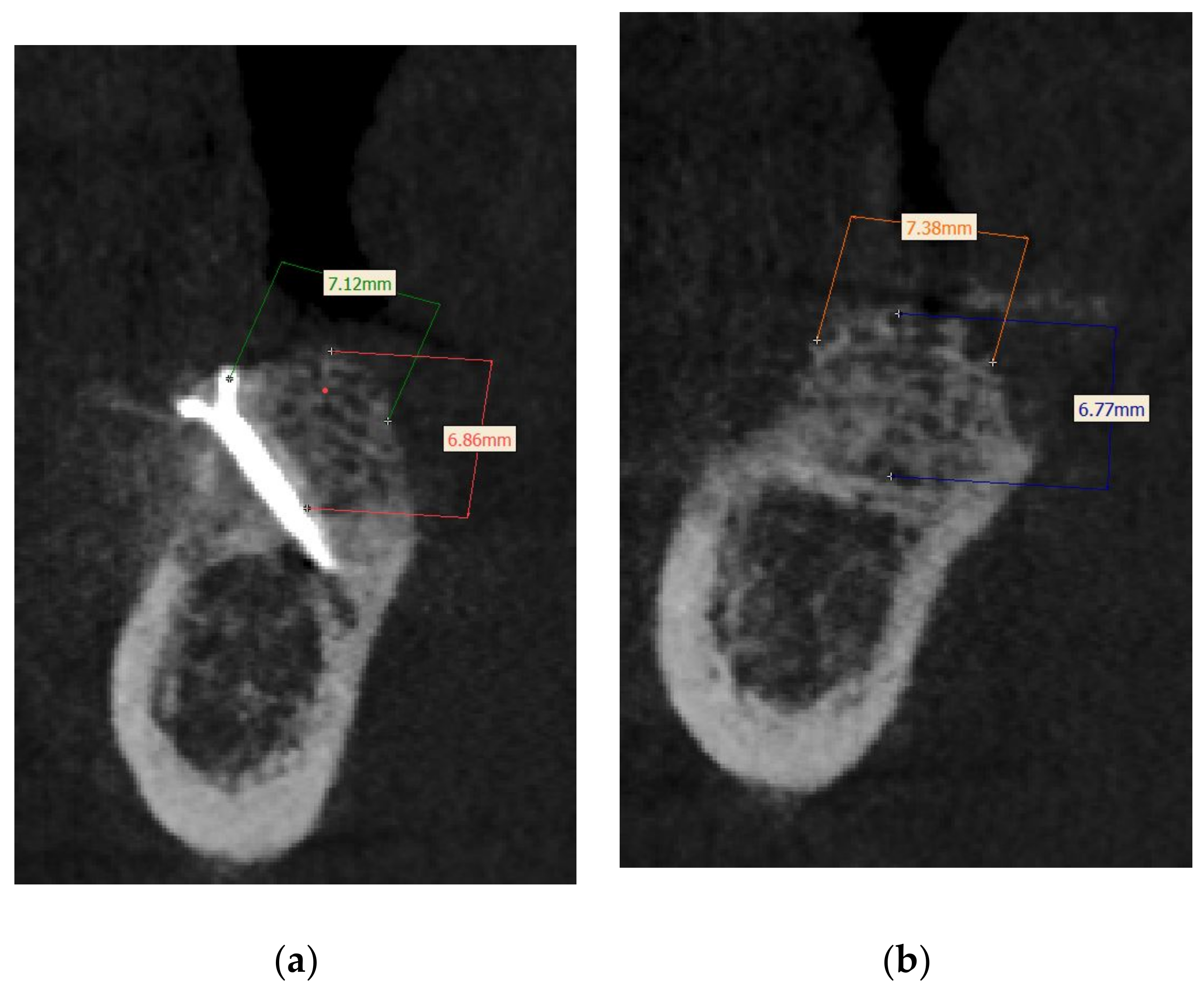
We were able to show an increase of the bone in the horizontal dimension of 7.38 mm and at a vertical height of 6.86 mm (Figure 12a,b).
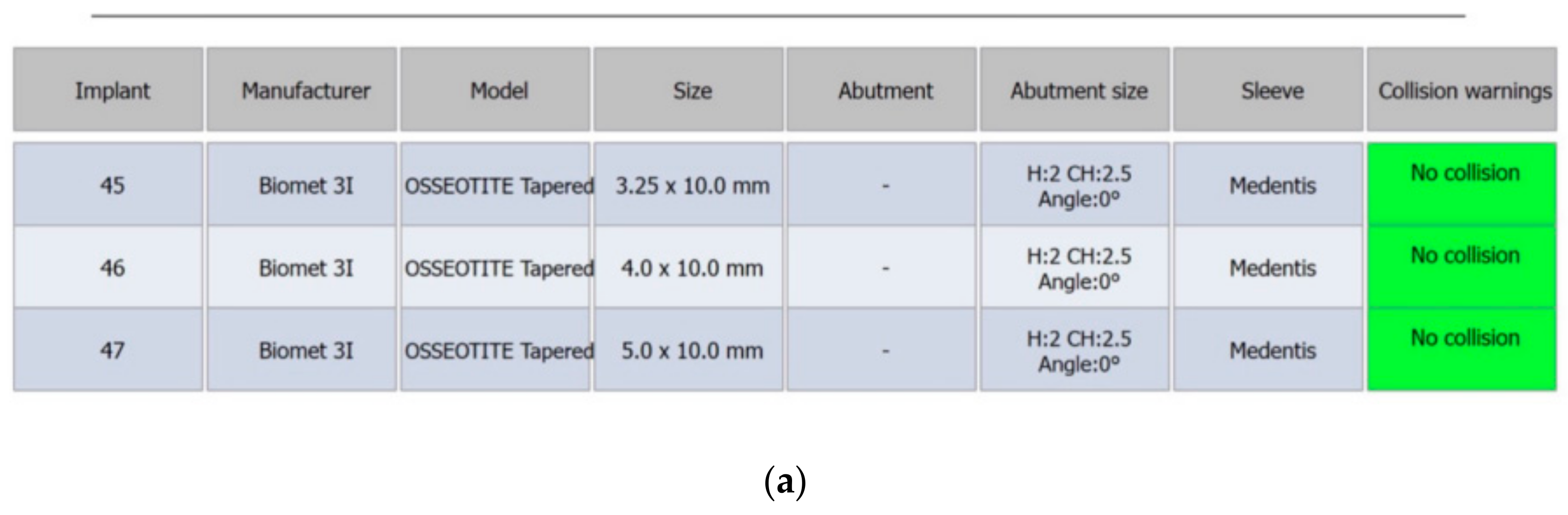
The previous failed implant was left submerged to avoid the potential risks of nerve damage or need of additional grafting. Three implants were planned with a diameter of 3.25–5.0 mm and a length of 10 mm (Figure 13a–c).
7. Implant Placement
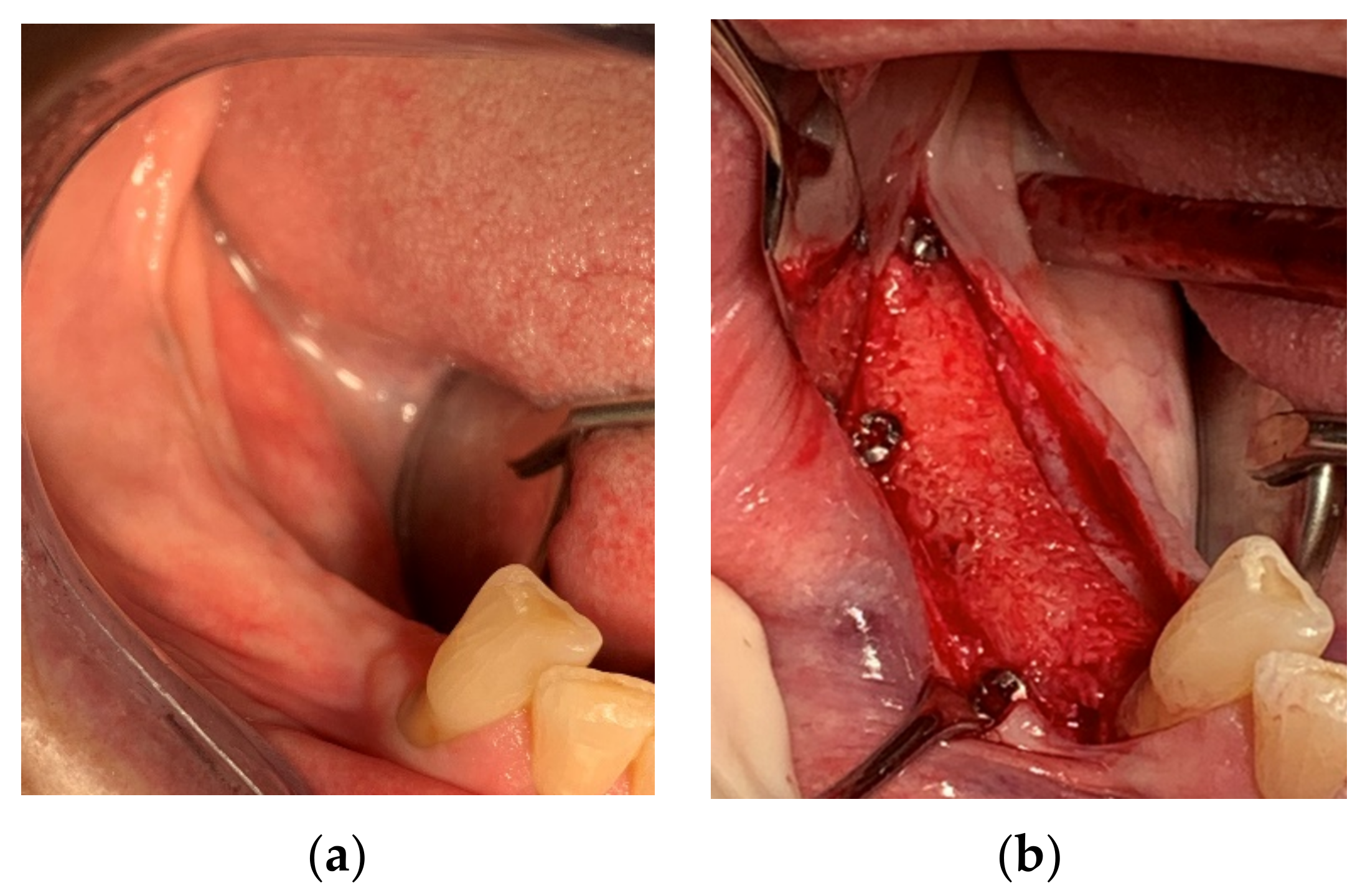
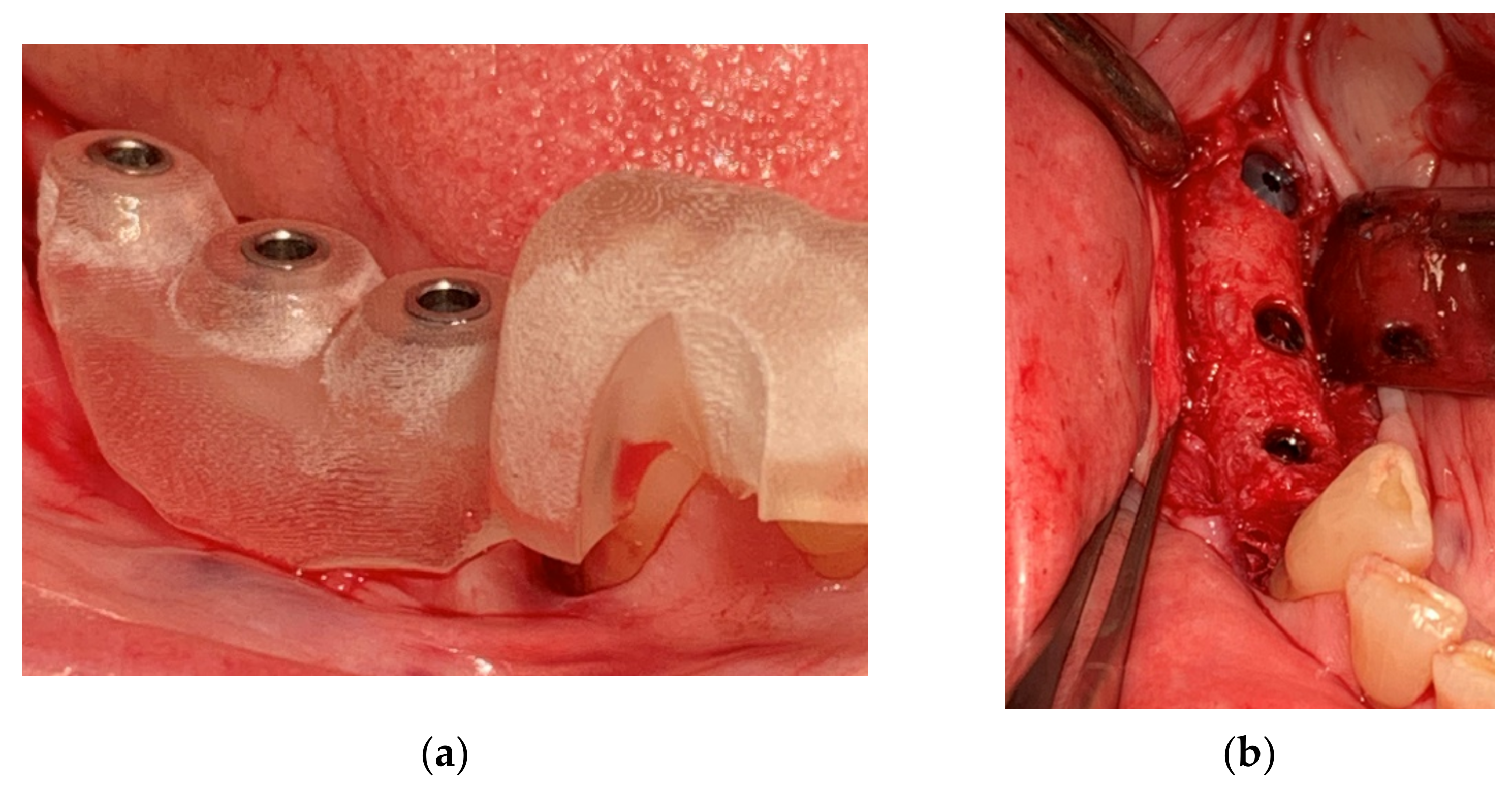
After 6 months of healing, a full-thickness flap was performed, and the screws to retain the ACBB were removed (Figure 14a,b). Three implants were placed with platform switching (Biomet 3i, T3 implants), according to the implant planning, using a surgical (prosthetic) guide. The implants were placed 1mm subcrestally, and a Puros Dermis® Allograft soft tissue matrix (Zimmer Biomet Dental) was placed over the implants to improve the thin tissue phenotype (Figure 15a,b and Figure 16).
8. Histology
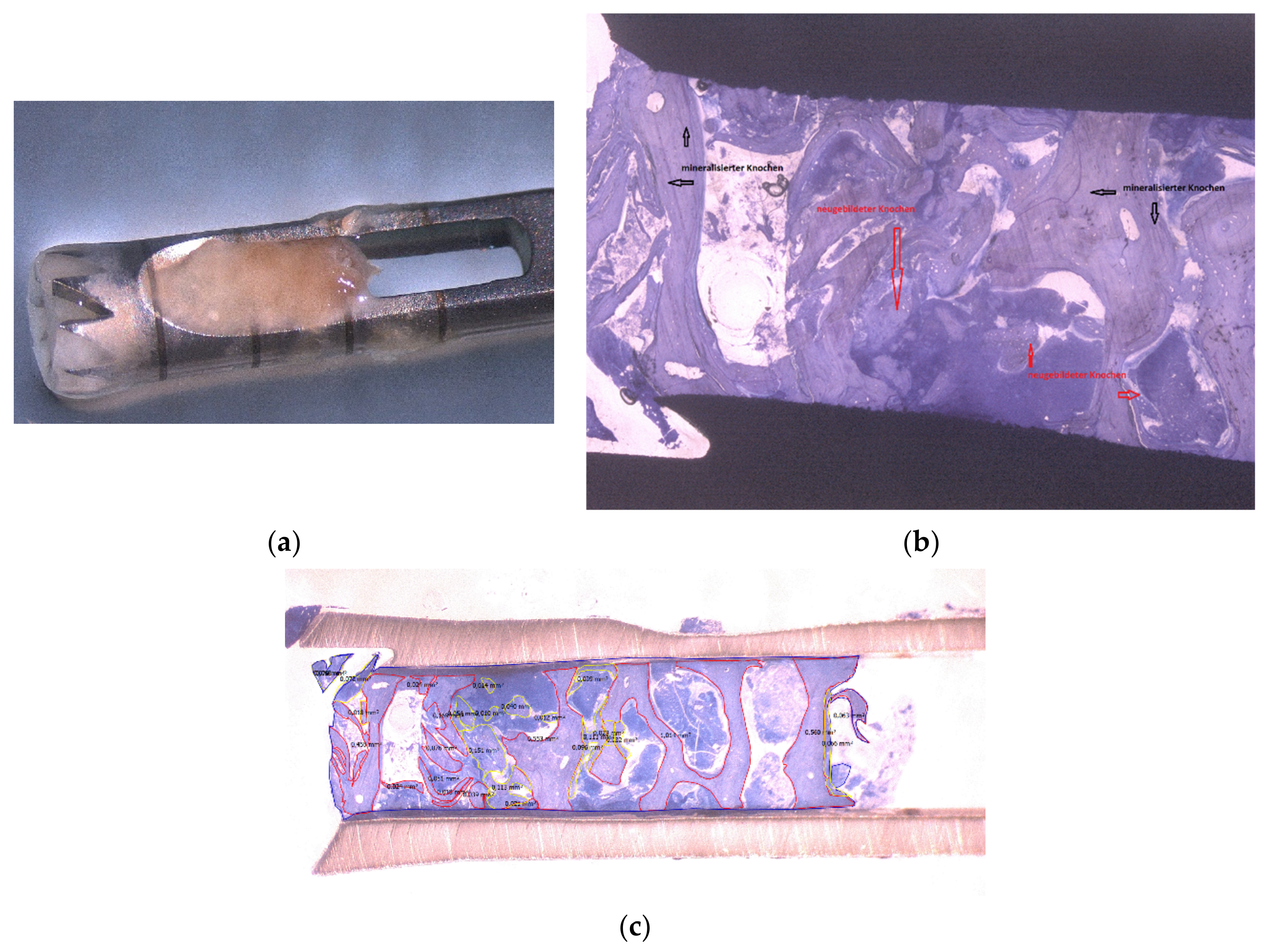
A 6-mm biopsy of the ACBB was taken at implant site #31 using a 2.8-mm diameter trephine. The trephine with the harvested bone was fixed in a neutral-buffered formalin 4% solution. The histological specimen was prepared following the method by Donath and Breuner [16,17], colored with Toluidine blue, and photographed with a Leica DM1000 camera (DFC 320, Software: Leica Application Suite).
9. Prosthetic Treatment
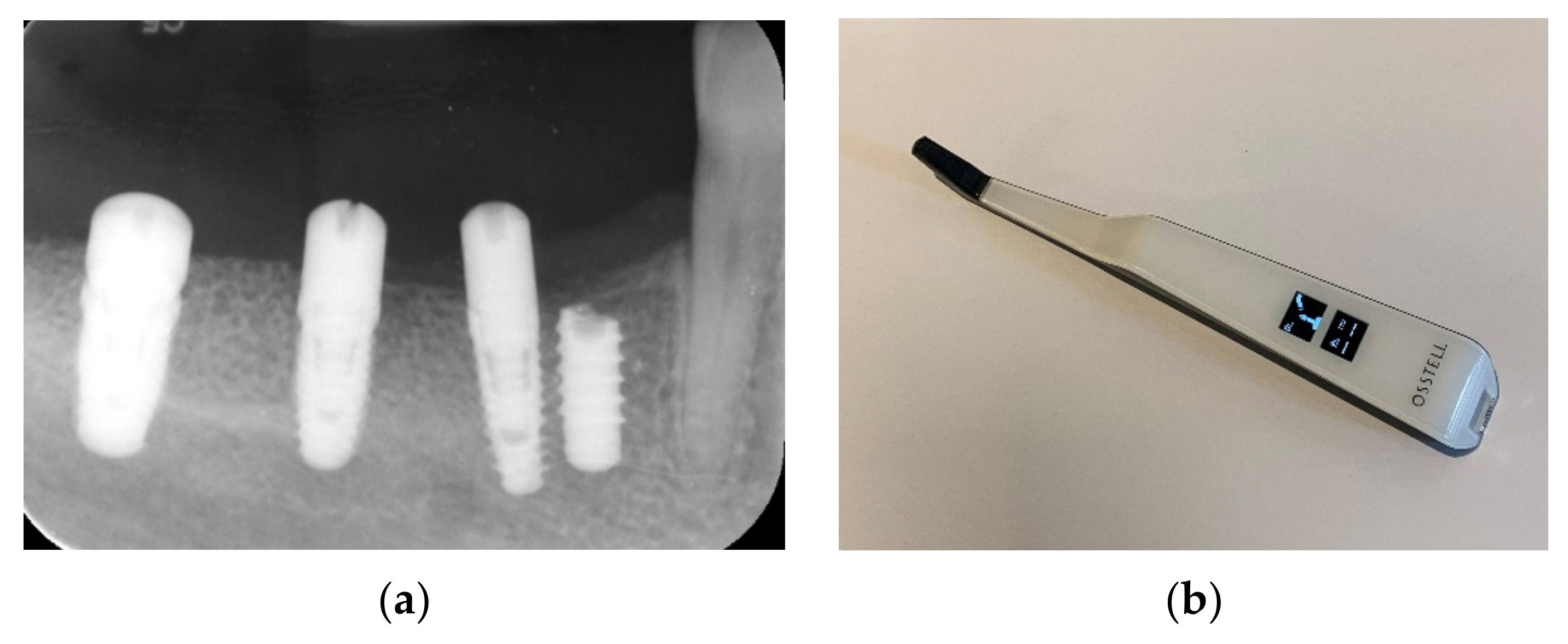
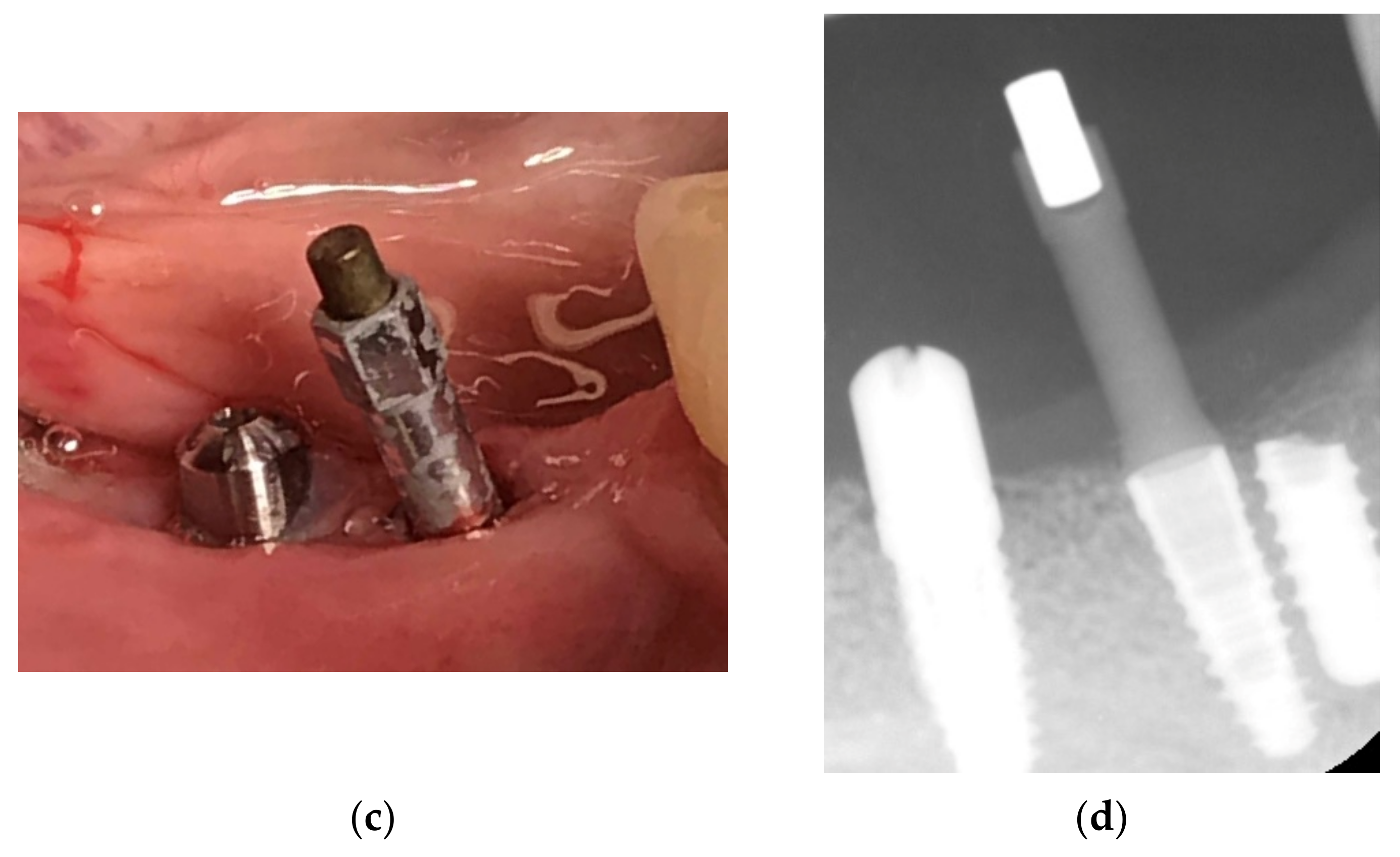
After 3 months of osseointegration, healing abutments were placed, and the implant stability was evaluated with a resonance frequency analysis (RFA) and ISQ values utilizing the Osstell device, showing great implant stability (Table 1) (Figure 18a–d).
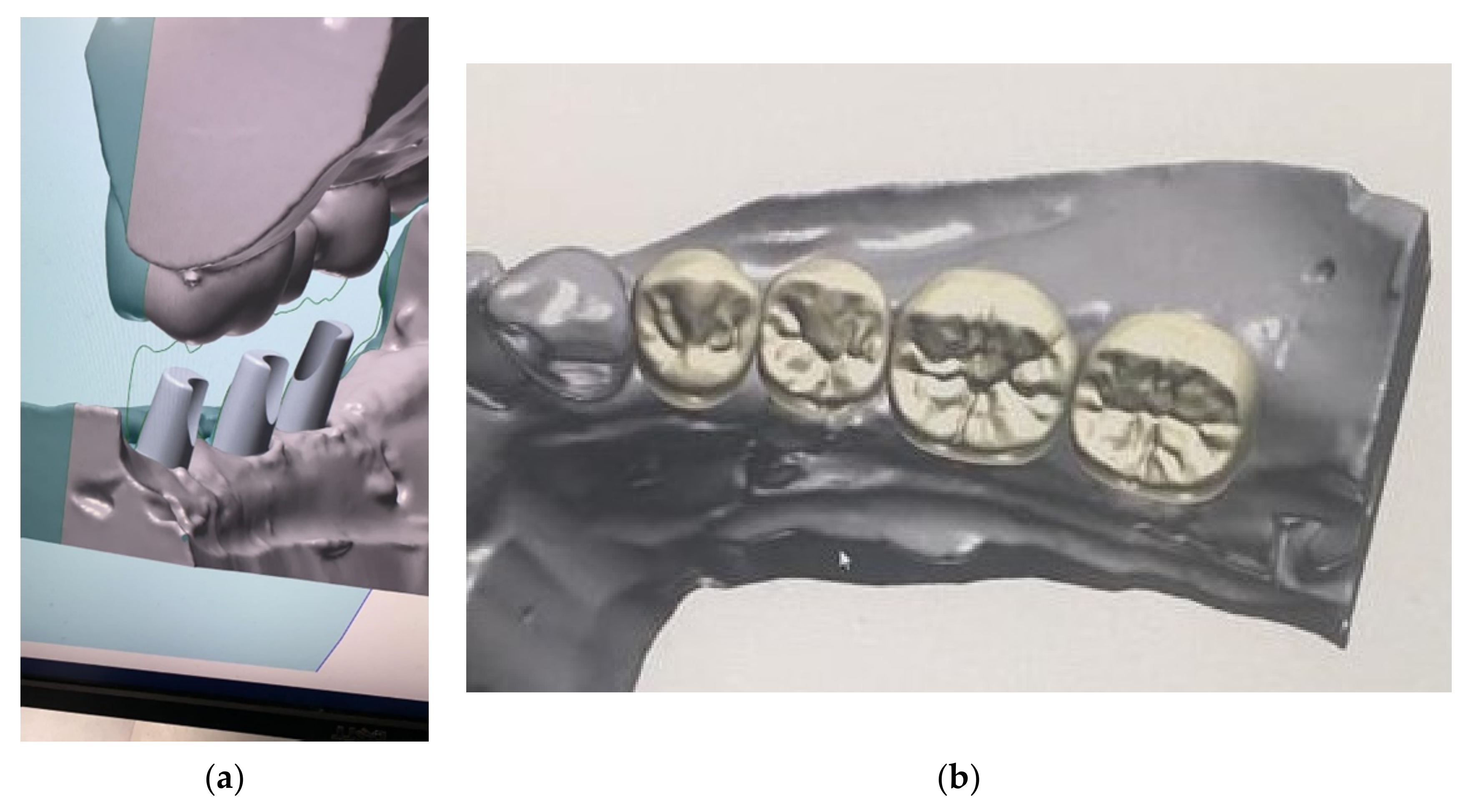
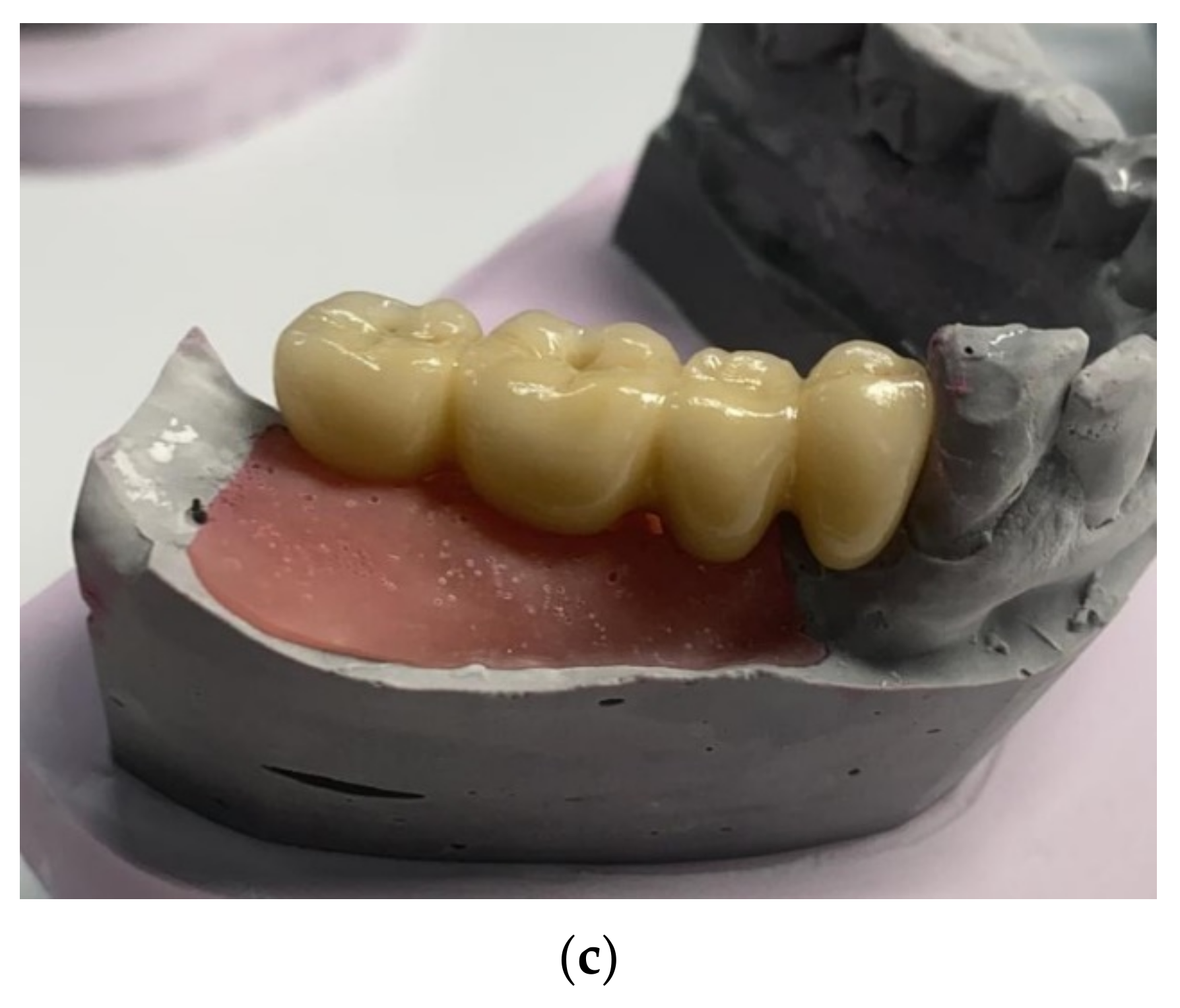
Impressions were taken using an open impression tray. The abutments were individually designed, and the bridge was made with a zirconia structure and baked porcelain for a screw-retained cantilever bridge. The bridge was delivered and screwed on at 30–35 Ncm 4 months after implant placement (Figure 19a–c) and, in total, ten months after placement of the allograft customized bone block, showing an excellent esthetic result. Teflon tape was placed over the screws to establish retrievability. The Teflon was covered finally with a composite to improve the esthetic clinical outcome (Figure 20a,b).
10. Follow-Up
11. Discussion
Autogenous bone is often considered the “gold standard” material for bone augmentation procedures, with proven results [18,19]. However, there are still controversial results regarding the long-term results after grafting with autogenous bone blocks. Significant graft resorption between 20% and 100% of the grafted volume might occur and should be taken into consideration, as shown earlier [20,21]. In addition, clinical trials comparing autogenous grafts with bone substitutes observed no differences for the clinical outcomes [1]. Tutoplast®-processed bone allografts are widely used and have been studied extensively [22,23,24,25,26]. Up to 127% more vital bone formation has been found after sinus grafting with allograft particulates compared to sinuses that have been grafted with a non-resorbable xenograft material [24,27]. The amount of residual grafting material after 6 to 7 months of healing time is low, confirming the active remodeling of the allograft material, which seems to be completed after 11 months [28]. Comparing Tutoplast-processed bone allograft to other freeze-dried allografts, it has been shown that, after several months of healing time, the bone formation is higher and amount of residual allograft particulates is lower for Tutoplast-processed bone allografts [29,30].
The use of allogeneic bone blocks for facial reconstruction was firstly described by Converse in 1950 [31]. Since then, allograft bone blocks have been compared with autogenous bone blocks in a variety of studies. Laino et al. showed comparable bone formations when using Tutoplast®-processed allograft blocks compared to autogenous blocks in vertical defects in the posterior mandible [32]. Comparable implant survival and success rates of dental implants placed in autogenous block or allograft block-grafted sites have been published [33,34]. Kim et al. showed a minimal resorption and high-volume stability of 94.3 ± 5.45% after allograft block grafting [35]. Schlee and coworkers focused on esthetic results after treating patients with autogenous and allograft blocks. Their results showed no differences in the Pink Esthetic Score (PES) between both groups [36]. Moreover, patients assessed the allograft procedure as less painful, since no second site surgery was needed to harvest a block [36]. However, for both types of block grafts, either autogenous blocks or pre-shaped allograft blocks, chairside manipulation is required to fit the block to the defect site, which results in increased surgery time and patient morbidity [37]. Finally, the fit of a manually shaped block graft will never be optimal, which might impact the revascularization and integration of the graft [37].
Customized allograft bone blocks may be beneficial due to their precise fit, which results in a reduced surgery time and risk of complications [3,4,34]. The shape of the block allows for a precise outcome in bone height and width, which is more random when using grafting techniques with particulate materials. The large contact surface area of the block improves in the growth of blood vessels and revascularization [37]. Puros® Allograft Customized blocks have shown bone remodeling and integration after six months of healing and stable results in different indications and clinical reports [4,38,39]. Apart from the fit of the graft, the defect site preparation might have an influence on the integration and vascularization of the block graft. Tresguerres and coworkers showed that cortical perforation of the recipient site did not influence the angiogenesis and new bone formation compared to nonperforated sites [40]. In this presented case report, there was uneventful healing, resulting in minimal to no volume loss of the customized allograft bone block 5 months after placement, and the histology after 6 months showed 46.61% mineralized bone, similar to the previous published results [40]. After three months of healing, the implant stability showed ISQ values over 70. In the present clinical case, a 6-month maturation time before implant placement was maintained, and after implant placement, an additional period of 3 months allowed for healing following the traditional healing protocol to allow increased maturation of the bone graft [7]. Following this surgical protocol, no loss of volume was observed after 5 months. Guided implant surgery using computer-designed stereolithographic guides is a reliable technique when the mean accuracy is taken into account, but if the maximum deviation is taken into account, the same technique appears far from accurate. Clinicians should be alert near vital structures, and a minimum of at least 2 mm from these anatomical structures should be respected [41]. These new techniques are often described as risk-free and easy to use. Computer-guided implantology does not overcome all limitations and should only be used by the experts to improve the results. A typical “learning curve” effect was not identified for static computer-assisted implant surgery [42].
This is one case report with a 15-month follow-up. In the literature, only one article had a 5-year follow-up. In this article, they took a biopsy, and it showed a well-vascularized lamellar bone with fatty incorporations without any avital allograft remnants. The presence of osteocytes, lining the cell macrophages and blood vessels, indicated healthy and vital one tissue [6]. More research is necessary to confirm the results of the used customized allograft bone blocks for the rehabilitation of the resorbed posterior mandible.
12. Conclusions
The present clinical case report of an allograft customized bone block presents a good and stable solution to vertical bone augmentation in a severely atrophic mandible. The key to the successful placement of the customized bone block was sufficient flap advancement and tissue management. An adequate flap release is necessary to perform a tension-free flap closure to avoid complications and bone resorption. The bone block needs to be rehydrated to improve the ductility and reduce the risk of a fracture.
Author Contributions
Conceptualization, M.J.B.; writing—original draft preparation, M.J.B.; writing—review and editing, G.E.R.; surgery, M.J.B.; visualization, M.J.B.: and supervision, G.E.R. All authors have read and agreed to the published version of the manuscript.
Funding
This case report did not receive any external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was given by the patient.
Acknowledgments
The CBCT analysis and allograft bone block design were performed by Stefan Berger, and the prosthetic work was done by Roland Boorsma, RB Dentaldesign, The Netherlands.
Conflicts of Interest
The authors declare that there were no conflicts of interest.
References
- Romanos, G.E. Severely Atrophy of the Posterior Mandible and Inferior Alveolar Nerve Transposition. Int. J. Periodontics Restor. Dent. 2021, 41, e199–e204. [Google Scholar] [CrossRef] [PubMed]
- Jacotti, M.; Barausse, C.; Felice, P. Posterior Atrophic Mandible Rehabilitation with Onlay Allograft Created with CAD-CAM Procedure: A Case Report. Implant Dent. 2014, 23, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlee, M.; Rothamel, D. Ridge augmentation using customized allogenic bone blocks: Proof of concept and histological findings. Implant Dent. 2013, 22, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blume, O.; Back, M.; Born, T.; Smeets, R.; Jung, O.; Barbeck, M. Treatment of a bilaterally severely resorbed posterior mandible due to early tooth loss by Guided Bone Regeneration using customized allogeneic bone blocks: A case report with 24 months follow-up data. J. Esthet. Restor. Dent. 2018, 30, 474–479. [Google Scholar] [CrossRef]
- Blume, O.; Donkiewicz, P.; Back, M.; Born, T. Bilateral maxillary augmentation using CAD/CAM manufactured allogenic bone blocks for restoration of congenitally missing teeth: A case report. J. Esthet. Restor. Dent. 2019, 31, 171–178. [Google Scholar] [CrossRef]
- Kloss, F.R.; Offermanns, V.; Donkiewicz, P.; Kloss-Brandstätter, A. Customized allogeneic bone grafts for maxillary horizontal augmentation: A 5-year follow-up radiographic and histologic evaluation. Clin. Case Rep. 2020, 8, 886–893. [Google Scholar] [CrossRef] [Green Version]
- Landsberg, C.; Moses, O. Ridge Augmentation Using Customized Allogeneic Bone Block: A 3-Year Follow-up of Two Case Reports. Int. J. Periodontics Restor. Dent. 2020, 40, 881–889. [Google Scholar] [CrossRef]
- Schoepf, C. Allograft Safety: The efficacy of the Tutoplast Process. Int. Mag. Oral Implantol. 2006, 1, 10–15. [Google Scholar]
- Romanos, G.E. Periosteal Releasing Incision for Successful Coverage of Augmented Sites. A Technical Note. J. Oral Implantol. 2010, 36, 25–30. [Google Scholar] [CrossRef]
- Ronda, M.; Stacchi, C. Management of a coronally advanced lingual flap in regenerative osseous surgery: A case series introducing a novel technique. Int. J. Periodontics Restor. Dent. 2011, 31, 505–513. [Google Scholar]
- Keith, J.D.; Petrungaro, P.; Leonetti, J.A.; Elwell, C.W.; Zeren, K.J.; Caputo, C.; Nikitakis, N.G.; Schopf, C.; Warner, M.M. Clinical and histologic evaluation of a mineralized block allograft: Results from the developmental period (2001–2004). Int. J. Periodontics Restor. Dent. 2006, 26, 321–327. [Google Scholar]
- Leonetti, J.A.; Koup, R. Localized maxillary ridge augmentation with a block allograft for dental implant placement: Case reports. Implant Dent. 2003, 12, 217–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanos, G. Anatomical and Biologic Considerations of Autogenous Bone Blocks Harvested from the Ramus Region. Int. J. Oral Maxillofac. Implant. 2019, 34, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Park, J.S.; Lim, S.C. Placement of implant after bone graft using J block allograft. Implant Dent. 2010, 19, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Schlee, M. Augmentation with a customized milled bone graft. Digit. Dent. News 2013, 3, 40–48. [Google Scholar]
- Donath, K. The diagnostic value of the new method for the study of undecalcified bones and teeth with attached soft tissue (Sage-Schliff (sawing and grinding) technique). Pathol. Res. Pract. 1985, 179, 631–633. [Google Scholar] [CrossRef]
- Donath, K.; Breuner, G. A method for the study of undecalcified bones and teeth with attached soft tissues. The Sage-Schliff (sawing and grinding) technique. J. Oral Pathol. 1982, 11, 318–326. [Google Scholar]
- Khoury, F.; Hanser, T. Three-Dimensional Vertical Alveolar Ridge Augmentation in the Posterior Maxilla: A 10-year Clinical Study. Int. J. Oral Maxillofac. Implant. 2019, 34, 471–480. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Mascellaro, A.; Ferrario, S.; Beretta, M. Dental implants placed in resorbed alveolar ridges reconstructed with iliac crest autogenous onlay grafts: A 26-year median follow-up retrospective study. J. Cranio Maxillofac. Surg. 2019, 47, 805–814. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Guidetti, F.; Califano, L.; Bufo, P.; Sbordone, L. Volume changes of autogenous bone after sinus lifting and grafting procedures: A 6-year computerized tomographic follow-up. J. Cranio Maxillofac. Surg. 2013, 41, 235–241. [Google Scholar] [CrossRef]
- Wiltfang, J.; Jatschmann, N.; Hedderich, J.; Neukam, F.W.; Schlegel, K.A.; Gierloff, M. Effect of deproteinized bovine bone matrix coverage on the resorption of iliac cortico-spongeous bone grafts—A prospective study of two cohorts. Clin. Oral Implant. Res. 2014, 25, e127–e132. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Finger, I.; Lytle, R. Human mineralized bone in extraction sites before implant placement: Preliminary results. J. Am. Dent. Assoc. 2002, 133, 1631–1638. [Google Scholar] [PubMed]
- Noumbissi, S.S.; Lozada, J.L.; Boyne, P.J.; Rohrer, M.D.; Clem, D.; Kim, J.S.; Prasad, H. Clinical, histologic, and histomorphometric evaluation of mineralized solvent-dehydrated bone allograf (Puros) in human maxillary sinus grafts. J. Oral Implantol. 2005, 31, 171–179. [Google Scholar] [PubMed]
- Froum, S.J.; Wallace, S.S.; Elian, N.; Cho, S.C.; Tarnow, D.P. Comparison of mineralized cancellous bone allograft (Puros) and anorganic bovine bone matrix (Bio-Oss) for sinus augmentation: Histomorphometry at 26 to 32 weeks after grafting. Int. J. Periodontics Restor. Dent. 2006, 26, 543–551. [Google Scholar]
- Tsao, Y.P.; Neiva, R.; Al-Shammari, K.; Oh, T.J.; Wang, H.L. Effects of a mineralized human cancellous bone allograft in regeneration of mandibular Class II furcation defects. J. Periodontol. 2006, 77, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Brown, D.; Wang, H.L. Sandwich bone augmentation for predictable horizontal bone augmentation. Implant Dent. 2009, 18, 282–290. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Doering, H.; Schmidt, T.; Lutz, R.; Neukam, F.W.; Schlegel, K.A. Histological results after maxillary sinus augmentation with Straumann(R) BoneCeramic, Bio-Oss(R), Puros(R), and autologous bone. A randomized controlled clinical trial. Clin. Oral Implant. Res. 2013, 24, 576–585. [Google Scholar] [CrossRef]
- Soardi, C.M.; Suarez-Lopez del Amo, F.; Galindo-Moreno, P.; Catena, A.; Zaffe, D.; Wang, H.L. Reliability of Cone Beam Computed Tomography in Determining Mineralized Tissue in Augmented Sinuses. Int. J. Oral Maxillofac. Implant. 2016, 31, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Monje, A.; O’Valle, F.; Monje-Gil, F.; Ortega-Oller, I.; Mesa, F.; Wang, H.L.; Galindo-Moreno, P. Cellular, Vascular, and Histomorphometric Outcomes of Solvent-Dehydrated vs Freeze-Dried Allogeneic Graft for Maxillary Sinus Augmentation: A Randomized Case Series. Int. J. Oral Maxillofac. Implant. 2017, 32, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Silva, F.; Lipton, D.; Tanello, B.; Duarte, W.; Witek, L.; Coelho, P.G.; Neiva, R. Clinical, Radiographic, and Histologic Comparison of Regular Mineralized and Tutoplast-derived Allograft for Alveolar Ridge Preservation. In Proceedings of the Academy of Osseointegration Annual Meeting 2019, Washington, DC, USA, 13–16 March 2019. [Google Scholar]
- Converse, J.M. Restoration of facial contour by bone grafts introduced through the oral cavity. Plast. Reconstr. Surg. 1950, 6, 295–300. [Google Scholar]
- Laino, L.; Iezzi, G.; Piattelli, A.; Lo Muzio, L.; Cicciu, M. Vertical ridge augmentation of the atrophic posterior mandible with sandwich technique: Bone block from the chin area versus corticocancellous bone block allograft—Clinical and histological prospective randomized controlled study. Biomed. Res. Int. 2014, 2014, 982104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motamedian, S.R.; Khojaste, M.; Khojasteh, A. Success rate of implants placed in autogenous bone blocks versus allogenic bone blocks: A systematic literature review. Ann. Maxillofac. Surg. 2016, 6, 78–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacotti, M.; Wang, H.L.; Fu, J.H.; Zamboni, G.; Bernardello, F. Ridge augmentation with mineralized block allografts: Clinical and histological evaluation of 8 cases treated with the 3-dimensional block technique. Implant Dent. 2012, 21, 444–448. [Google Scholar] [CrossRef]
- Kim, S.J.; Shin, H.S.; Shin, S.W. Effect of bone block graft with rhBMP-2 on vertical bone augmentation. Int. J. Oral Maxillofac. Surg. 2010, 39, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Schlee, M.; Dehner, J.-F.; Baukloh, K.; Happe, A.; Seitz, O.; Sader, R. Esthetic outcome of implant-based reconstructions in augmented bone: Comparison of autologous and allogeneic bone block grafting with the pink esthetic score (PES). Head Face Med. 2014, 10, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAllister, B.S.; Haghighat, K. Bone augmentation techniques. J. Periodontol. 2007, 78, 377–396. [Google Scholar] [CrossRef] [Green Version]
- Engler-Hamm, D. Komplexe Rehabilitation mit CAD/CAM-Knochenblöcken: Auswertung mittels DVT nach 0, 6 und 21 Monaten. Implantologie 2018, 26, 231–242. [Google Scholar]
- Gedrange, T.; Dominiak, M. Orthodontic splint treatment of patients with limited bone supply. Ger. Med. J. 2018, 23, 44–53. [Google Scholar]
- Tresguerres, F.G.F.; Tresguerres, I.F.; Iglesias, O.; Leco, I.; Tamimi, F.; Torres, J. The role of cortical perforations in allogeneic block grafting for lateral augmentation in maxilla: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2021, 1–13. [Google Scholar] [CrossRef]
- Cassetta, M.; Stefanelli, L.V.; Giansanti, M.; Di Mambro, A.; Calasso, S. Accuracy of a computer-Aided Implant Surgical Technique. Int. J. Periodontics Restor. Dent. 2013, 33, 317–325. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F.; Giansanti, M.; Bellardini, M.; Brandetti, G.; Piccoli, L. Is there a learning curve in static computer-assisted implant surgery? A prospective clinical study. Int. J. Oral Maxillofac. Surg. 2020, 49, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Clinical situation: bone deficiency in the right posterior mandible.

Figure 2.
Panoramic radiograph showing the implant planning and nerve position.

Figure 3.
Position of the CBCT slice (a) showing the exact location of the canal (b).

Figure 4.
(a,b) Bone block design.

Figure 5.
Flap advancement for sufficient cover of the bone block.

Figure 6.
Size of the ACBB (a) and hydration of the bone block (b).

Figure 7.
Bone block fixated with TruFix screws (a) and covered with Copioss (b).

Figure 8.
Postoperative radiograph (a) and clinical condition after flap closure (b).

Figure 9.
Follow-up after two weeks.

Figure 10.
Surgical site of the mandible before (a) and 5 months after surgery (b).

Figure 11.
(a–c) CBCT analyses showing the results vs. design (yellow lines).

Figure 12.
(a,b) The results in bone gain in width and height.

Figure 13.
(a–c) Implant planning.


Figure 14.
Clinical view before implant placement (a) and a full-thickness flap showing fixation (b).
Figure 14.
Clinical view before implant placement (a) and a full-thickness flap showing fixation (b).

Figure 15.
Drill guide (a) and implants in place (b).

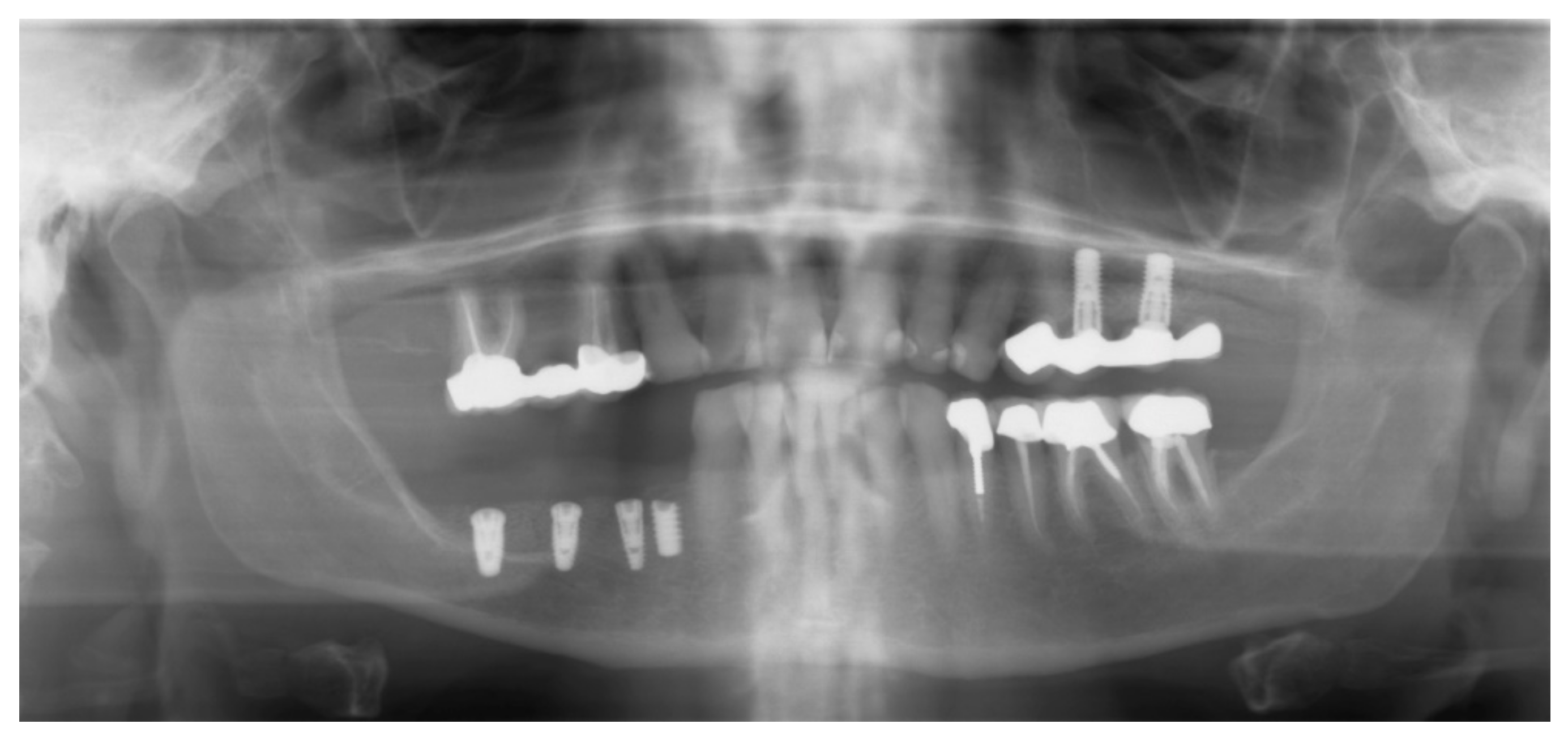
Figure 16.
Panoramic radiograph showing the implants in place.

Figure 17.
Trephine drill with bone biopsy (a) and histology photos (b,c). The results showed new bone formation (yellow) and structures of mineralized (ACCB) bone (red) after 6 months of healing, as expected.
Figure 17.
Trephine drill with bone biopsy (a) and histology photos (b,c). The results showed new bone formation (yellow) and structures of mineralized (ACCB) bone (red) after 6 months of healing, as expected.

Figure 18.
Stability ISQ measurements (a–d).


Figure 19.
Prosthetic planning and design (a–c).


Figure 20.
Bridge delivery (a) and control radiograph (b).

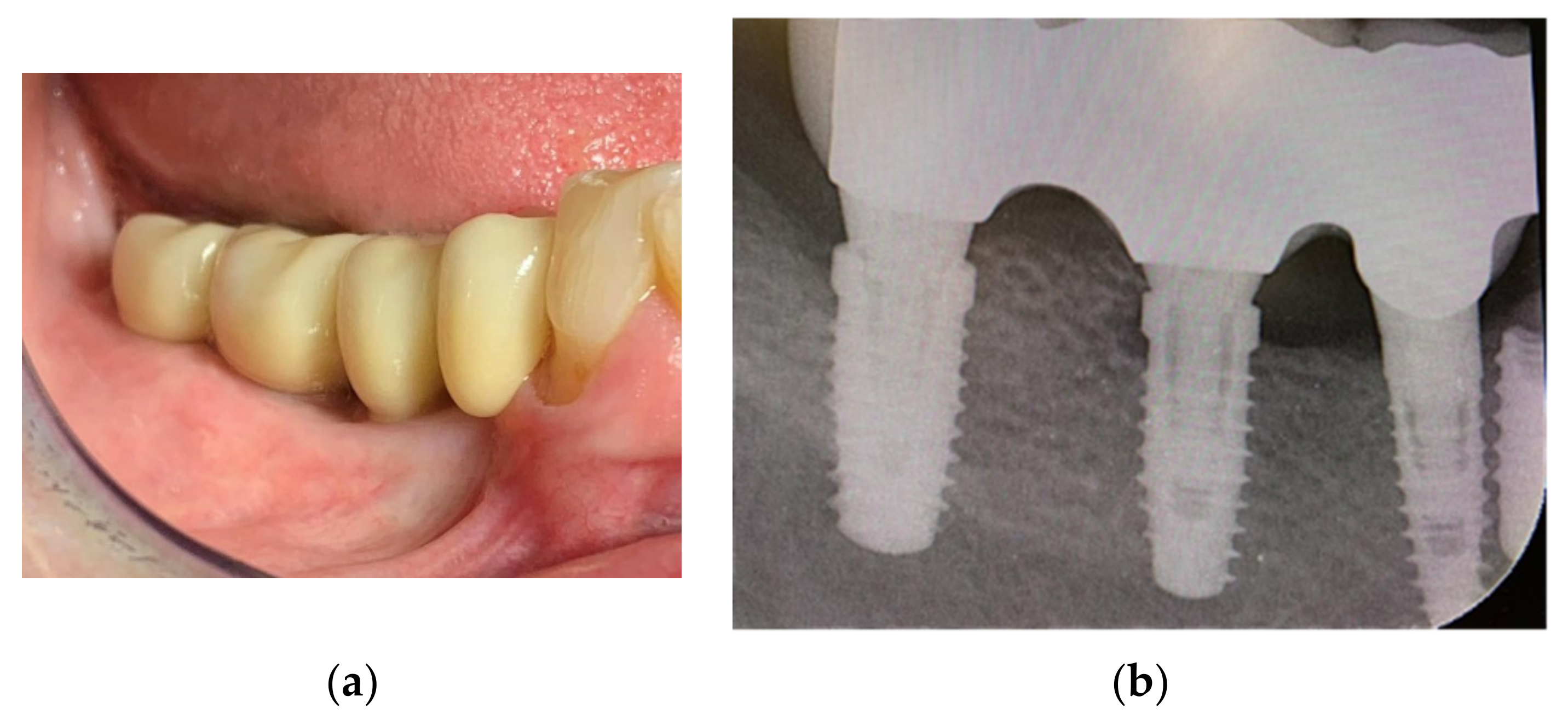
Figure 21.
Follow-up at 15 months: clinical view (a) and control radiograph (b).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Insertion torque and ISQ values.
| Implant Site (#) | Insertion Torque | ISQ Values |
|---|---|---|
| 29 | 25 Ncm | 73 |
| 30 | 50 Ncm | 83 |
| 31 | 50 Ncm | 86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Boogaard, M.J.; Romanos, G.E. Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis. Appl. Sci. 2021, 11, 10413. https://doi.org/10.3390/app112110413
AMA Style
Boogaard MJ, Romanos GE. Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis. Applied Sciences. 2021; 11(21):10413. https://doi.org/10.3390/app112110413
Chicago/Turabian StyleBoogaard, Maarten J., and Georgios E. Romanos. 2021. "Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis" Applied Sciences 11, no. 21: 10413. https://doi.org/10.3390/app112110413
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.