
WIC Staff Views and Perceptions on the Relationship between Food Insecurity and Perinatal Depression

 ,
,  ,
, {kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. Data Collection and Data Analysis
2.3. Ethical Approval
2.4. WIC Clinic Staff Participants
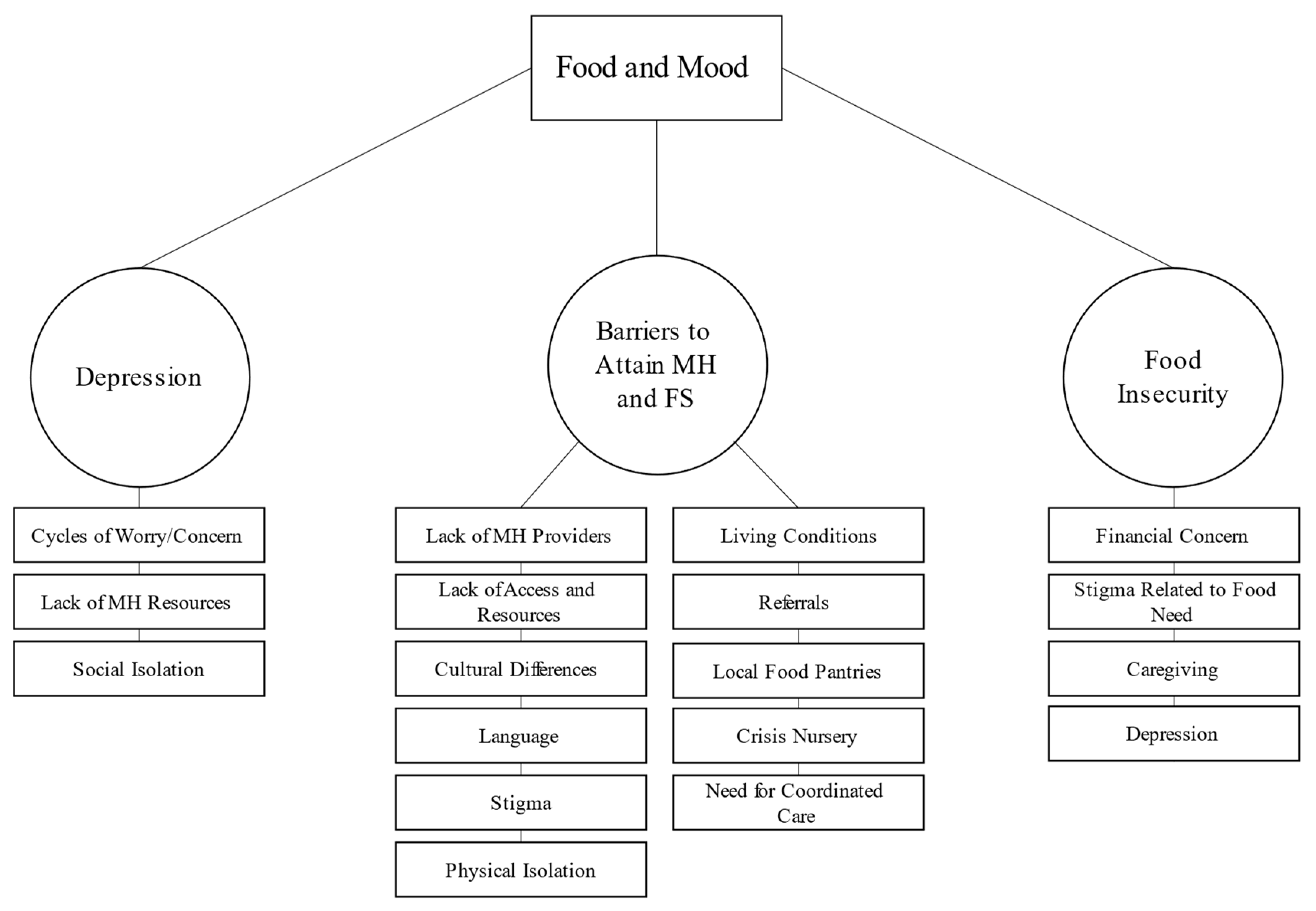
3. Results
3.1. Depression Experienced by Perinatal WIC Clients
“It’s like a cloud … They don’t see clear[ly] what’s going on … they need to [care for their family] … but they don’t have the energy. It’s not just affecting them; it’s affecting the whole family.”
It goes to all those … daily stressors, every single day. So if … you are constantly worried about not having enough money, not having enough food, not having transportation. All of those things. And that feeds into depression and anxiety. It takes every single thing you have to get out of bed in the morning and get here. And maybe some days it’s not an option to get [to WIC] because you can’t.
It’s a hopelessness isolation ... I feel like the moms sense they don’t have food but [they don’t] have that urgency ... mentally. Mom can [go] through severe ... postpartum depression ... with good family support [but] they are feeling very isolated. They could have 10,000 people around [but they] encapsulate themselves, [so they] cannot really sense ... what’s surrounding them. It’s a protection ... mechanism. I see that a lot ... A lot of women do not speak [the] language, [and are] without transportation. They have to depend on [their] husband [to] drive them but [he] can be stuck in school ... I have [a mom] that experience[s] quite severe [depression], and she doesn’t even feed her baby. She doesn’t even remember the baby ... I mean you think rationally she loves her baby. She knows what she needs to do, but that’s what I [am] working [on] with her ... In my mind, [I] think about it like a lonely island. She’s there and ... she cannot see [a] way out. And then ... you can have so many people around her but that loneliness is very real to her.
3.2. Food Insecurity in Perinatal WIC Clients
“In order to eat healthy like you’re supposed to, you’re supposed to eat six times a day … three good meals, three good snacks. These women don’t have that. They are lucky if they get one meal.”
Even [if] they get coupons, they don’t have transportation [to] take them to the big supermarket to get the fresh produce. And that’s a hinder[ence] to access healthier food because they may have no transportation to get them to the big market where have more choice of fresh produce than if they go to little convenience store nearby the corner ... You drive through some ... low-income areas- you don’t see a green grocer but you see lots of convenience stores so those they’ll eat [those] foods. It’s not what’s ideal for their health. So that’s another thing I see. You can’t access food. The disparity is in ... accessing it because they don’t have transportation.
It’s very shameful to have to go somewhere ... and feel like you are begging for [food]. And if you get judged by somebody, then you really feel bad. And somebody ... might have had a bad situation before they came [to WIC where they] asked for food and [were] treated bad. So they’re very cautious about talking to somebody about getting food.
3.3. Barriers Preventing Perinatal WIC Clients from Attaining Food Security and Necessary Mental Health Services
“...[n]ot every agency accepts the medical card or ... does ... free based counseling without pay or sliding fee scale.”
We will call to try to make referrals for these women to our OBs … they will get denied access because the OBs don’t have knowledge of how to treat [women experiencing mental illness] and or they will start to treat them and they will call us and say we have got to discharge them because we just can’t handle their needs.
“...she was saying … ‘you don’t want to look poor, you don’t want anyone to perceive you as poor’ … [so] a lot of the time their stuff is … a smoke screen.”
… she’s opening her pantries asking me, can I eat this? Can I eat that? And it was like … American food. They gave her the ingredients to make tacos. She pulled the sour cream out [and asked] ‘can I eat this?’ [I said] [n]o you don’t eat that, you put it on things. But the assumption was made that she would know how to cook tacos with it.
[They will say] ‘I’m about to…be evicted from my apartment. There’s no food in the apartment. The power’s off. My refrigerator doesn’t work anyway because I don’t have any power …’ What takes precedence? So you know we can zero in on food. We can do something about that in most cases, but the other stuff is harder.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coleman-Jensen, A.; Rabbitt, M.; Gregory, C.; Singh, A. Household Food Security in the United States in 2014; Economic Research Service: Washington, DC, USA, 2014. [Google Scholar]
- Hromi-Fiedler, A.; Bermúdez-Millán, A.; Segura-Pérez, S.; Pérez-Escamilla, R. Household food insecurity is associated with depressive symptoms among low-income pregnant Latinas. Matern. Child Nutr. 2011, 7, 421–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharkey, J.R.; Johnson, C.M.; Dean, W.R. Relationship of Household Food Insecurity to Health-Related Quality of Life in a Large Sample of Rural and Urban Women. Women Health 2011, 51, 442–460. [Google Scholar] [CrossRef] [Green Version]
- Noonan, K.; Corman, H.; Reichman, N.E. Effects of maternal depression on family food insecurity. Econ. Hum. Biol. 2016, 22, 201–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezzeddin, N.; Jahanihashemi, H.; Zavoshy, R.; Noroozi, M. The Prevalence of Postpartum Depression and Its Association with Food Insecurity among Mothers Referring to Community Health Centers. Iran. J. Psychiatry 2018, 13, 280–287. [Google Scholar]
- Nagahawatte, T.; Goldenberg, R.L. Poverty, maternal health, and adverse pregnancy outcomes. Ann. N. Y. Acad. Sci. 2008, 1136, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.-Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Women's Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmans, R.S.; Berger, L.M.; Palta, M.; Robert, S.A.; Ehrenthal, D.B.; Malecki, K. Participation in the Supplemental Nutrition Assistance Program and maternal depressive symptoms: Moderation by program perception. Soc. Sci. Med. 2018, 197, 1–8. [Google Scholar] [CrossRef]
- Cook, J.T.; Black, M.; Chilton, M.; Cutts, D.; Ettinger de Cuba, S.; Heeren, T.C.; Rose-Jacobs, R.; Sandel, M.; Casey, P.H.; Coleman, S.; et al. Are food insecurity's health impacts underestimated in the U.S. population? Marginal food security also predicts adverse health outcomes in young U.S. children and mothers. Adv. Nutr. 2013, 4, 51–61. [Google Scholar] [CrossRef] [Green Version]
- Behimehr, S.; Curtis, D.; Curtis, R.; Hart, C. Perceived Healthcare Providers’ Responsibility with Postpartum Depression Whose Problem Is It, Anyway? J. Reprod. Med. 2014, 59, 139–144. [Google Scholar]
- Metallinos-Katsaras, E.; Gorman, K.S.; Wilde, P.; Kallio, J. A longitudinal study of WIC participation on household food insecurity. Matern. Child Health J. 2011, 15, 627–633. [Google Scholar] [CrossRef]
- Metallinos-Katsaras, E.; Must, A.; Gorman, K. A longitudinal study of food insecurity on obesity in preschool children. J. Acad. Nutr. Diet. 2012, 112, 1949–1958. [Google Scholar] [CrossRef] [PubMed]
- Maynard, M.; Andrade, L.; Packull-McCormick, S.; Perlman, C.M.; Leos-Toro, C.; Kirkpatrick, S.I. Food insecurity and mental health among females in high-income countries. Int. J. Environ. Res. Public Health 2018, 15, 1424. [Google Scholar] [CrossRef]
- Garg, A.; Toy, S.; Tripodis, Y.; Cook, J.; Cordella, N. Influence of maternal depression on household food insecurity for low-income families. Acad. Pediatr. 2015, 15, 305–310. [Google Scholar] [CrossRef]
- Sidebottom, A.C.; Hellerstedt, W.L.; Harrison, P.A.; Hennrikus, D. An examination of prenatal and postpartum depressive symptoms among women served by urban community health centers. Arch. Women's Ment. Health 2014, 17, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.C.L.; Dáu, A.L.B.T.; Goldblum, J.; Alfano, J.; Smith, M.V. A mixed methods investigation of the experience of poverty among a population of low-income parenting women. Community Ment. Health J. 2017, 53, 832–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browne, J.; Ponce, A. Assessing Food Insecurity in Individuals with Serious Mental Illness: A Pilot Training for Community Mental Health Providers. Community Ment. Health J. 2020, 56, 1110–1114. [Google Scholar] [CrossRef] [PubMed]
- Gundersen, C.; Engelhard, E.E.; Crumbaugh, A.S.; Seligman, H.K. Brief assessment of food insecurity accurately identifies high-risk US adults. Public Health Nutr. 2017, 20, 1367–1371. [Google Scholar] [CrossRef] [Green Version]
- Adams, E.; Hagunani, D.; Hoffmann, L.; Blaschke, G.; Helm, J.; Koehler, A. Screening for Food Insecurity in Pediatric Primary Care: A Clinic’s Positive Implementation Experiences. J. Health Care Poor Underserved 2017, 28, 24–29. [Google Scholar] [CrossRef]
- Ferrer, R.L.; Neira, L.-M.; De Leon Garcia, G.L.; Cuellar, K.; Rodriguez, J. Primary Care and Food Bank Collaboration to Address Food Insecurity: A Pilot Randomized Trial. Nutr. Metab. Insights 2019, 12, 1178638819866434. [Google Scholar] [CrossRef] [Green Version]
- Steiner, B.D.; Wahrenberger, J.T.; Raney, L. Providing effective primary care for patients with serious mental illness: Additional components to enhance practice. Community Ment. Health J. 2020, 56, 592–596. [Google Scholar] [CrossRef]
- Saxe-Custack, A.; Lofton, H.C.; Hanna-Attisha, M.; Victor, C.; Reyes, G.; Ceja, T.; LaChance, J. Caregiver perceptions of a fruit and vegetable prescription programme for low-income paediatric patients. Public Health Nutr. 2018, 21, 2497–2506. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabb, K.M.; Simonovich, S.D.; Wozniak, J.D.; Barton, J.M.; Hsieh, W.-J.; Klement, C.; Ostrowski, M.E.; Lakhani, N.; Meline, B.S.; Huang, H. WIC Staff Views and Perceptions on the Relationship between Food Insecurity and Perinatal Depression. Healthcare 2023, 11, 68. https://doi.org/10.3390/healthcare11010068
Tabb KM, Simonovich SD, Wozniak JD, Barton JM, Hsieh W-J, Klement C, Ostrowski ME, Lakhani N, Meline BS, Huang H. WIC Staff Views and Perceptions on the Relationship between Food Insecurity and Perinatal Depression. Healthcare. 2023; 11(1):68. https://doi.org/10.3390/healthcare11010068
Chicago/Turabian StyleTabb, Karen M., Shannon D. Simonovich, Jana D. Wozniak, Jennifer M. Barton, Wan-Jung Hsieh, Claire Klement, Mary Ellen Ostrowski, Noreen Lakhani, Brandon S. Meline, and Hsiang Huang. 2023. "WIC Staff Views and Perceptions on the Relationship between Food Insecurity and Perinatal Depression" Healthcare 11, no. 1: 68. https://doi.org/10.3390/healthcare11010068